Charu Tiwari, Kiran Khedkar, Shalika Jayaswal, Hemanshi Shah.
Department of Pediatric Surgery, TNMC & BYL Nair Hospital, Mumbai, India.
ADDRESS FOR CORRESPONDENCE
Dr Hemanshi Shah, Professor and HOD, Department of Pediatric Surgery, TNMC & BYL Nair Hospital, Mumbai 400008, Maharashtra, India.
Email: hemanshisshah@gmail.com | | Abstract | | Burkitt’s lymphoma is a highly malignant and rapidly growing B-cell neoplasm. Its presentation as intussusception is rare. We describe four children with intussusception due to Burkitt’s lymphoma. Three of them presented with abdominal pain and lump; had intussusception with a lead point on abdominal ultrasound (USG). They were managed by emergency exploration and resection of the involved bowel with anastomosis. Histopathological diagnosis was Burkitt’s lymphoma. The fourth patient presented with abdominal pain, a huge abdominal lump and fever. He had two previous episodes of recurrent intussusceptions managed by USG-guided hydrostatic reduction. This time, he was diagnosed as Burkitt’s lymphoma by image guided biopsy and started on appropriate chemotherapy. | | | | Keywords | | Intussusception, recurrent, Burkitt’s lymphoma, children. | | | | Introduction | | Burkitt’s lymphoma, first described by Dennis Burkitt in 1958, is a highly malignant, aggressive and rapidly growing form of Non-Hodgkin lymphoma (NHL). It usually presents as malignant lesions in extra nodal sites or as an acute leukemia. (1) Three variants have been described – endemic, sporadic and immunodeficiency associated. The endemic form is more common and is seen in Africa. It presents as tumor of jaw or other facial bones and is associated with Epstein Barr virus (EBV) as well as frequent concomitant malaria infection. The sporadic form is less common but is seen worldwide and commonly presents as acute abdomen and abdominal mass involving the terminal ileum, caecum or mesentery; atypical presentation mimicking acute appendicitis may be seen.(2) Intussusception caused by Burkitt lymphoma as a cause of acute abdomen is rare, with often misleading symptoms that make the diagnosis more difficult.(2) In up to 18% of patients presenting with primary abdominal Burkitt lymphoma, intussusception is the presenting feature.(3) Many pediatric patients with Burkitt lymphoma present with intussusception as a first clinical sign, a presentation that potentially leads to the disease detection at an earlier stage.(4) We present 4 children who presented with intussusception and were diagnosed to have Burkitt’s lymphoma. | | | | Case Report | Four children who presented with intussusception and were later diagnosed to be Burkitt’s lymphoma on histopathology are described.
The mean age at presentation was 6.25 years. Two were males and two were females. Three of them presented with abdominal pain and a non-tender lump at umbilical region and intussusception with a lead point was diagnosed on ultrasonography (USG). The duration of their symptoms was 1 month, 1 week and 2 months with aggravation of symptoms since 6 days respectively. The child with duration of 6 days was tried barium reduction fluoroscopically but was unsuccessful. At exploration, all these three patients had a mass as the lead point (one had a caecal polyp). The mass along with the diseased bowel was resected and anastomosis was done. The enlarged mesenteric lymph nodes were biopsied. The histopathological diagnosis was Burkitt’s lymphoma with clear surgical margins. (Figure 1) Only one had involvement of the mesenteric lymph node. In all these three patients, 2 courses of chemotherapy were administered with excellent outcome at 24 months after surgery.
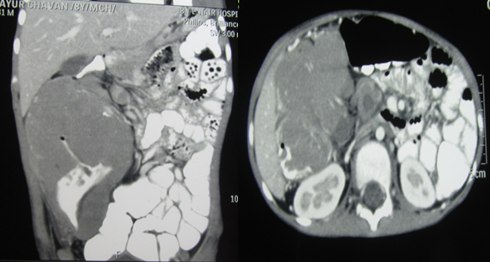
The fourth patient had two previous admissions with intussusception, which was reduced hydrostatically under USG guidance. Computed tomography was done second time in view of recurrent intussusception but it did not show any lead point. Third time he was admitted after 6 months with a huge right sided abdominal lump which on CT Scan was seen arising from the terminal ileum, caecum and ascending colon. (Figure 2) CT guided biopsy suggested Burkitt’s lymphoma and the patient is at present under chemotherapy (Intravenous cyclophosphamide, vincristine, doxorubicin; oral prednisolone and intrathecal methotrexate) and is responding to it.
Figure 1: Histopathology Image showing small round blue cells arranged in cords and sheets.
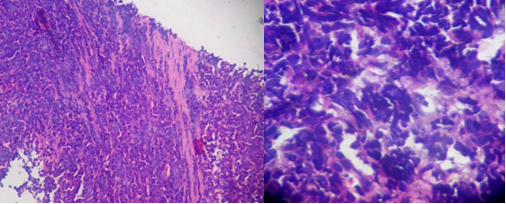
Figure 2 (a) & (b): Computed Tomography scan of the fourth patient showing large bulky concentric mass involving the terminal ileum, caecum and ascending colon and multiple enlarged necrotic peri colic and mesenteric lymph nodes.
 | | | | Discussion | Intussusception is one of the most common pediatric surgical emergency which requires prompt diagnosis and appropriate non-operative or operative intervention. Intussusception occurs throughout the world with an incidence of approximately 1 to 4 in 2000 infants and children with males outnumbering females by 2:1 or 3:2 ratio.(5) Although intussusception can be seen in all pediatric ages from prenatal to the late teens, 75% of cases occur within the first 2 years of life and 90% in children within 3 years of age.(5) Especially in older children, i.e., in the rest 10% of the cases, there is a pathological lesion (Meckel’s diverticulum, polyp, and lymphoma) at the lead point of the intussusceptum.(4,6-8) Ultrasonography, when combined with clinical examination, is approximately 100% diagnostic for intussusception.(6) Barium enema, CT and colonoscopy can also be helpful in diagnosis.(9) Recurrent intussusception can occur in up to 20% of cases and most of these usually occur within 6 months of the first episode.(5) Most of the recurrent intussusceptions are managed by hydrostatic reduction. Surgery is indicated in cases of irreducible recurrences, perforations and pathological lead point causing recurrent intussusception. (5)
Primary gastrointestinal lymphoma represents 1-4% of all gastrointestinal malignancies.(10) The distal ileum or ileocecal region is most commonly involved in children.(11,12) Non-Hodgkin’s Lymphoma (NHL) is the third most frequent cancer of childhood and usually is subdivided into 3 histological subtypes: (a) 65% B-cell NHL including both Burkitt lymphoma and diffuse large B-cell lymphoma; (b) 20% lymphoblastic and (c) 15% anaplastic large cell lymphoma.(13,14) Burkitt lymphoma represents 40%-50% of all NHL cases in childhood and is more common in males than females. (12-14) Predisposing factors for lymphoma of the small intestine includes prior malabsorption syndromes, inflammatory bowel disease and immunodeficiency states. (12) These risk factors were absent in all of our patients who were previously healthy.
The presentation of undiagnosed Burkitt lymphoma is very non-specific, making the diagnosis difficult. (10) Abdominal pain is present in 80% of the cases of intussusception with Burkitt lymphoma, along with nausea, vomiting, constipation, diarrhea, fatigue or malaise. (4) The rapidity of volumetric doubling of this neoplasm frequently leads to an acute abdomen presentation that may mimic other diseases (bowel obstruction secondary to ileocecal intussusception caused by tumor growth, obstruction or bleeding; some presentations may mimic acute appendicitis). (2,9) In three of our cases, the patients presented with pain and lump abdomen and had intussusception and the fourth one had previous history of two episodes of intussusception recurrences.
The ideal treatment of gastrointestinal lymphoma must be individualized based on the type of disease and its location and a multidisciplinary approach with surgery and chemotherapy increases the chances of event free survival. (11-13) Surgery is needed for complete resection in limited disease, diagnostic biopsies, management of life-threatening local tumor effects and second-look operations.(13) Surgery can confirm the diagnosis and can relieve the common presenting symptoms of intestinal obstruction, abdominal mass, intussusception, or acute abdomen.(10) Complete resection is associated with improved survival.(2) Some reports demonstrate higher survival rate (58-89%) in patients having extensive surgical resection versus patients having only partial or incomplete resection (40-45%) at 2-5 years.(2)
Surgery also provides important prognostic information through definitive staging, offers a chance for cure by helping in planning adjuvant therapy and may prevent complications such as hemorrhage, obstruction or perforation. (11)
Burkitt lymphoma is very sensitive to chemotherapy (15); therapy courses include the following drugs: cyclophosphamide, methotrexate, cytarabine, iphosphamide, etoposide, vincristine, vindesine, adriamycin, doxorubicin, dexamethasone. (13,16) rituximab is currently being studied in clinical trials, because it has shown good results in adult NHL. (17) Although regimens are effective, they are toxic because up to 3% can die from treatment complications, with acute tumor lysis syndrome being one of them. (17) Burkitt lymphoma patients who present with intussusception require shorter-duration and less intense chemotherapy than patients diagnosed in other ways. (10) | | | | Conclusion | | Burkitt lymphoma is a highly malignant, rapidly growing and aggressive neoplasm that the pediatric surgeon should consider when faced with a child with a non-specific clinical presentation, who complains of diffuse abdominal pain, weight loss, and/or presents with recurrent intussusception. The suspicion of a pathological lesion lead point in the intussusception and presentation of the intussusception at ages beyond the normal often necessitates surgery. Surgery is the gold standard in both diagnosis and treatment, ensuring the excision of the entire tumor with free margins. A multidisciplinary team with an oncologist assures efficient therapeutic management. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Burkitt D. A sarcoma involving the jaws in African children. Br J Surg. 1958;46:218–223. [CrossRef] [PubMed]
- Hoxha FT, Hashani SI, Krasniqi AS, Kurshumliu FI, Komoni DS, Hasimja SM et al. Intussusceptions as acute abdomen caused by Burkitt lymphoma: a case report. Cases Journal. 2009, 2:9322. [CrossRef] [PubMed]
- Grajo JR, Kayton ML, Steffensen TS, Dragicevic N, Guidi CB. Presentation of Ileal Burkitt Lymphoma in Children. J Radiol Case Rep. 2012; 6(8): 27–38. [CrossRef]
- Gupta H, Davidoff AM. Clinical implications and surgical management of intussusception in pediatric patients with Burkitt lymphoma. J Pediatr Surg. 2007 Jun;42(6):998-1001; discussion 1001. [CrossRef] [PubMed]
- Young DG. Intussusception. In: O'Neil JA Jr, Rowe MI, Grosfeld JL, Fonkalsrud EW, Coran AG, eds. Pediatric Surgery. 5th ed. Mosby, New York, USA. 1998. p. 1185-98.
- Puri P, Höllwarth M, (compilers). In: Pediatric Surgery Diagnosis and Management. New York: Springer; 2009. pp. 485–490. [CrossRef]
- Hutson JM, O'Brien M, (compilers). In: Jones' Clinical Paediatric Surgery: Diagnosis and Management, 6th edition. Blackwell Publishing; 2008. pp. 126–129.
- Seifarth FG, Triana J. Diagnosis and laparoscopic treatment of ileoileal intussusception secondary to heterotopic pancreas in an infant: case report and review of the literature. J Pediatr Surg. 2011;46:33–36. [CrossRef] [PubMed]
- Aydede H, Sakarya A. Ileocolic intussusception due to ileal lymphoma (Case report). Turk J Gastroenterol. 2002;13:236–238. [PubMed]
- Bălănescu NR, Topor L, Malureanu D, Stoica I. Ileocolic intussusception due to Burkitt lymphoma: a case report. J Med Life. 2013; 6(1): 61–64. [PubMed]
- Chen CY, Wu CC. Primary non-Hodgkin's lymphoma of rectum presenting with rectal prolapse. J Pediatr Surg. 2009;44:1–3. [CrossRef] [PubMed]
- Erol MF, Karakayali AS. Mucosa-associated lymphoid tissue lymphoma of the ileum as the cause of an intestinal invagination. J Pediatr Surg. 2008;43:13–15. [CrossRef] [PubMed]
- Attarbaschi A, Mann G. The role of surgery in the treatment of pediatric B-cell non-Hodgkin's lymphoma. J Pediatr Surg. 2002;37:1470–1475. [CrossRef] [PubMed]
- Cogliati SB, Novak U. Diagnosis of Burkitt lymphoma in due time: a practical approach. Diagnostic Pathology. 2007;2:6. [CrossRef] [PubMed]
- Brichon P, Bertrand Y. Burkitt's lymphoma revealed by acute intussusception in children. Ann Chir. 2001;126:649–653. [CrossRef]
- Chieng JH, Garrett J, Ding SL, Sullivan M. Clinical presentation and endoscopic features of primary gastric Burkitt lymphoma in childhood, presenting as a protein-losing enteropathy: a case report. J Med Case Rep. 2009 Jun 9;3:7256. [CrossRef] [PubMed]
- Ehrlich PF. Hodgkin Lymphoma and Non-Hodgkin Lymphoma. In: O'Neil JA Jr, Rowe MI, Grosfeld JL, Fonkalsrud EW, Coran AG, (eds). Pediatric Surgery. 5th ed. Mosby, New York, USA. 1998. p. 1185-98.
DOI: https://doi.org/10.7199/ped.oncall.2016.39
|
| Cite this article as: | | Tiwari C, Khedkar K, Jayaswal S, Shah H. Burkitt`s Lymphoma Presenting as Intussusception in Four Children. Pediatr Oncall J. 2016;13: 71-73. doi: 10.7199/ped.oncall.2016.39 |
|