Marta Pelicano, Marta Figueiredo, Inês Pinto Ferreira
Serviço de Pediatria do Hospital de São Francisco Xavier, Centro Hospitalar Lisboa Ocidental, Lisboa, Portugal
Address for Correspondence: Marta Pelicano, Estrada Forte do Alto Duque, 1449-005, Lisboa.
Email: mpelicano@chlo.min-saude.pt
|
Question :A previously healthy 7-year-old male child was admitted to the emergency department presenting an acute onset of dyspnea and stridor preceded by a 2-day course of fever and cough. Physical examination revealed tachycardia, polypnea, audible stridor, peripheral oxygen saturation of 83%, chest wall retraction and pulmonary auscultation globally decreased breath sounds. Acute laryngotracheobronchitis was assumed. Supplemental oxygen, nebulized adrenaline, oral dexamethasone, salbutamol and methylprednisolone were administered, with poor response. Blood tests were performed (leukocytes 26000/µL; CRP 1,08 mg/dL) as well as an antero-posterior chest X-ray, showing the “Steeple sign” (Figure 1). The severity of the disease motivated the transfer to a Central Hospital with an Intensive Care Unit. Epiglottitis and Foreign body aspiration were excluded. Type A Influenza viruses was isolated and the patient received a 5 day-course of Oseltamivir as well as supportive measures, with favorable outcome.
Figure 1. “Steeple sign” - Antero-posterior chest X- ray demonstrates uniform narrowing of the subglottic airway. 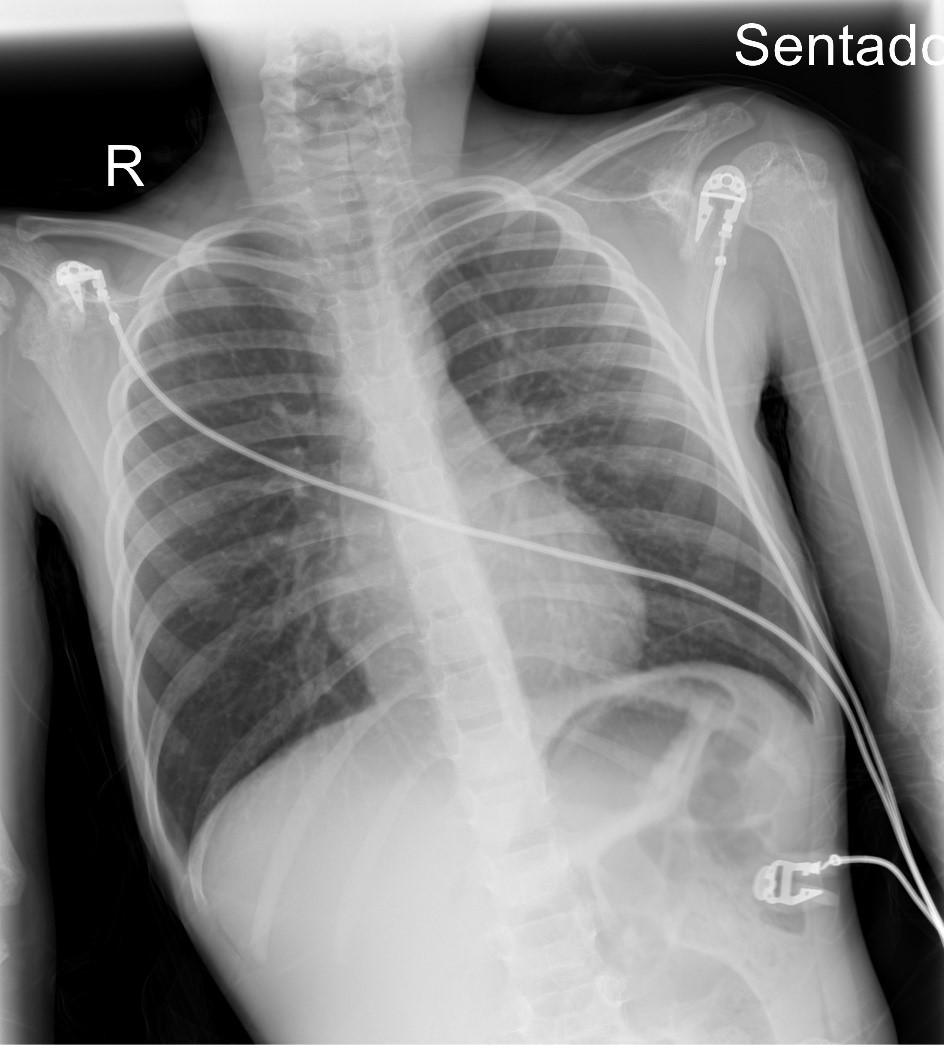 What is the diagnosis?
|
Discussion :
Acute laryngotracheobronchitis (Croup) is a viral infection of the upper airway that is characterized by inspiratory stridor, laryngeal cough and dysphonia. 1,2,3,4 Although it is a mild and self-limiting disease in most cases, rarely significant airway obstruction can occur and be fatal. 2,4 Therefore it is important that the Pediatrician recognizes early signs of severe obstruction, that indicate the need to refer to pediatric intensive care. 1,2,3
Typical radiographic findings include the “Steeple sign”, seen in antero-posterior neck or chest radiographs, demonstrating uniform narrowing of the subglottic airway, producing an inverted “V” appearance. A corresponding lateral X-ray would show narrowing of the subglottic airway, as well as the distention of the hypopharynx. 2,3,4,5 Although not specific and only present in about 50% of cases, in cases with severe presentation may reinforce the diagnosis and exclude other causes of airway obstruction (for example: radio-opaque foreign body). 2,3,4| References : | - Fernandez J, Sánchez A, Bonis A et al. Manual de Diagnóstico y terapéutica en Pediatría, 6ª Edicion, 2017. Laringitis, epiglotitis y traqueobronquitis. 142: 1365-1372.
- Woods CR. Croup: Clinical features, evaluation, and diagnosis. Uptodate, 2023.
- Ortiz-Alvarez O. Acute management of croup in the emergency department, 2017. Paediatrics & Child Health.22(3):166-173.
- Lars J Grimm. Croup Imaging. Medscape, 2021.
- Matsuura H, Shimanouchi Y. Steeple sign and acute laryngotracheobronchitis. QJM: An International Journal of Medicine, 2017.110:767.
|
|
| Correct Answers : |  100% 100% |
Last Shown : Nov 2024
|