Beatriz Henriques
1, Joana Victor Lage
1, Maria Lurdes Torre
1, Piedade Sande Lemos
21Pediatrics Department, Hospital Professor Doutor Fernando Fonseca, Lisbon, Portugal,
2Hospitais CUF Cascais e Tejo, Lisboa, Portugal
Address for Correspondence: Beatriz Henriques, Rua José Cipriano Silveira Machado nº9 3ºG; 2745-140 Queluz, Lisboa, Portugal.
Email: beatrizfer.henriques@gmail.com
Keywords : Infliximab, Psoriasis, Cronh’s disease.
Question: We present a 16-year-old male diagnosed with Crohn’s disease at the age of 9. Upon diagnosis, he exhibited severe and extensive disease, including fistulizing perianal disease (Paris Classification A1L3B3) and a Pediatric Crohn's Disease Activity Index (PCDAI) >30. He was treated with Azathioprine (2-2,5 mg/kg/day) and Infliximab (5 mg/Kg at weeks 0 and 3 and then with maintenance infusions given every 6-8 weeks), with significant improvement of bowel disease.
During the first four years of treatment, he experienced intermittent, self-limited erythematous, scaly plaques scattered over the body, which responded well to symptomatic treatment with emollients and topical corticosteroids.
Five years after diagnosis, due to worsening of the bowel disease, the Infliximab therapy was increased to 10 mg/kg every 6 weeks and the patient experienced an exacerbation of the cutaneous lesions, which became widespread, particularly concentrated around the skinfold areas and scalp, causing intense pruritus. The patient denied the introduction of any new medications or topical products prior to the onset of the dermatosis (Figures 1 and 2).
Figure 1. Erythematous and scaly papules/plaques in the inguinal eaxillar area.
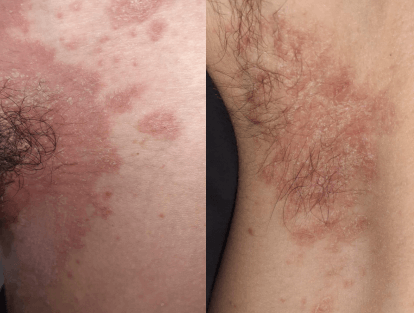 Figure 2.
Figure 2. Erythematous and scaly papules/plaques in the suprapubic area.

The patient reported worsening of these lesions after each Infliximab administration and due to the lack of improvement with symptomatic treatment, he was referred to a dermatology consultation. The biologic therapy was then switched to Ustekinumab leading to immediate improvement and complete resolution of the lesions six months after the therapeutic change.