Haemophilus influenzae type b complicated meningitis in an unimmunised immunocompetent child
Madara Grise
Riga Stradins University and Children Clinical University Hospital, Riga, Latvia
Address for Correspondence: Madara Grise, Riga Stradins University and Children Clinical University Hospital, Riga, Vienibas gatve 45, Riga LV-1004, Latvia.
Email: madara.grise@bkus.lv
Keywords: Haemophilus influenzae meningitis, Unimmunised child, Complicated meningitis
Clinical Problem :
Previously healthy, unimmunised, one year and ten months old boy with fever, breathing difficulties, vomiting and cough that had lasted for 4 days, was brought to the tertiary level university hospital after seizures and loss of consciousness.
Patient presented with symptoms of meningeal involvement, shock, GCS score 8/9 points and was admitted to paediatric intensive care unit (PICU).
Patient received intravenous Ceftriaxone 100 mg/kg, intravenous Vancomycin at the maximal dose for weight, intravenous acyclovir. White blood cell counts were 35148 cells per cubic millimetre of cerebrospinal fluid (CSF), with low Glucose levels (0.05 mmol/L) and elevated protein levels (1.82 g/L). Initial blood test results were WBC count, 9.17 × 10^3/mL; IL-6, 633 pg/mL; C-reactive protein (CRP), 243 mg/L. Brain magnetic resonance imaging (MRI) upon admission (5th day of the illness) showed a slightly accentuated leptomeningeal enhancement in the brain and around the distal part of the spinal cord. The blood levels of inflammatory markers began to decrease. Blood and cerebrospinal fluid culture results confirmed the presence of Ceftriaxone sensitive Hib.
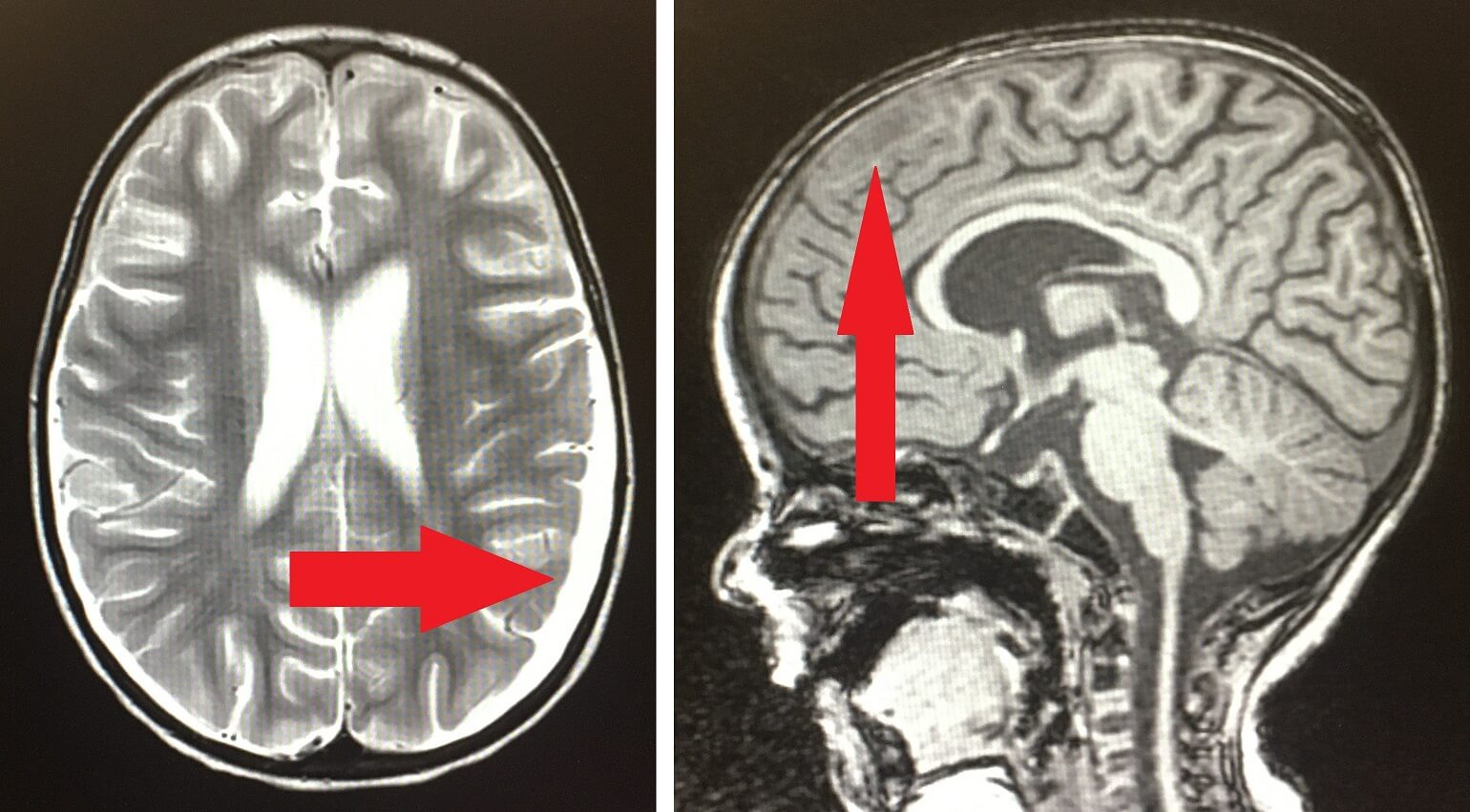
After 4 days in the PICU, the patient was transferred to an infectious disease ward. On the 10th day of illness, an increase of inflammatory markers was observed. The WBC count was 23 x10^3/mL, the IL-6 level was 371 pg/mL and the CRP level was 116 mg/mL (which continued to increase to 276 mg/L). Cultures were obtained from central and peripheral venous catheters, urine and stool samples. Chest radiography, ECG and echocardiography were performed to identify additional infection sources. Vancomycin was changed to piperacillin/tazobactam because of the existing risk of infection with multidrug-resistant intra-hospital microorganisms in the PICU. On the 11th day of illness, brain MRI showed complicated meningitis with subdural empyema around the frontal lobes, ventriculitis in the occipital horns and partial sinus transversus thrombosis on the left side. After changing the therapy, the inflammatory indicators initially decreased (IL-6 decreased to 96 pg/mL, CRP to 173 mg/L) until they re-elevated on the 15th day of illness. CRP levels increased to 235 mg/L and IL-6 to 159 pg/mL. The haemoglobin levels decreased to 6.4 mg/dL. Patients’ family initially refused blood transfusion but were persuaded to consent to transfusion of 1 red cell unit. On the 15th day of illness, repeat brain MRI showed sterile subdural effusion in the left parietal, occipital and temporal lobes and a small subdural empyema in both frontal lobes (Figure 1).
Figure 1. Brain MRI on the 15th day of illness (left) and on the 35th day of illness (right).
The dose of Ceftriaxone was increased to 250 mg/kg and Rifampicin 20 mg/kg was added to the therapy as a synergist. After the antibacterial therapy was intensified, on the 21st day of illness, MRI of the brain showed no increase in empyema, even more pronounced contrast of the membranes and resolved sinus transversus thrombosis.
In several weeks body temperature returned to normal. Inflammatory marker levels returned to normal around 34th day of illness. On the 35th day of illness brain MRI showed disappearance of subdural empyema, but oedema and signs of cerebritis were observed (Figure 1). Antibacterial therapy with Ceftriaxone and Rifampicin was continued for 6 weeks.
Patient partially regained motor skills approaching pre-illness state. Contrast of the soft membranes and wide lateral ventricles were observed in MRI on the 49th day, but no signs of cerebritis.
On the 51st day patient was discharged in good overall condition with following recommendations: brain MRI after 3 months, anticonvulsant therapy for =6 months, sleep EEG after 3 to 4 months and vaccination according to immunisation schedule. Parents were informed about the long-term neurological and cognitive outlook.
|
How long can therapy for complicated Hib infection last?
Discussion :
Risk factors for developing life-threatening Hib infections include children aged <5 years with incomplete immunisation against Hib, HIV infection, anatomic or functional asplenia, humoral immunodeficiencies, chemotherapy or radiation therapy. 1
After initiating adequate therapy, fever usually lasts for 3-6 days. 2 Fever can last for <5 days in approximately 10-15% of patients and recurrence of fever after being afebrile for 24 hours can occur in 15-20% of patients. 2,3 The causes of secondary or persistent fever include inadequate treatment or the development of nosocomial infections, also suppurative complications (subdural empyema, pneumonia, pericarditis or arthritis). The discontinuation of Dexamethasone can also cause secondary or persistent fever. 2
The duration of antibacterial therapy for simple Hib meningitis is 7-10 days, for complicated cases, it can be prolonged depending on the clinical course and diagnostic findings. 4
In case of complicated Hib meningitis, the use of Rifampicin is not common and this case report shows an example of a successful outcome with a combination of Ceftriaxone and Rifampicin treatment.
MRI was used repeatedly to monitor complications such as subdural empyema, cerebral vascular thrombosis and cerebritis. Other possible complications are brain abscesses and hydrocephalus. 5 The most common sequelae of bacterial meningitis are hearing loss, seizures, intellectual disability, spasticity and/or paresis. 6 As in the presented case, patients in shock or comatose, requiring mechanical ventilation, have increased mortality 7 and more difficult treatment.
Expert’s opinion
The treatment of bacterial meningitis can be complicated and very lengthy. Rifampicin can be used in combination with Ceftriaxone in the treatment of Hib meningitis as a synergistic agent. Vaccination can be initiated before hospital discharge. | References : | - Briere EC, Rubin L, Moro PL, et al. Prevention and control of haemophilus influenzae type b disease: recommendations of the advisory committee on immunization practices (ACIP). MMWR Recomm Rep. 2014;63(RR-01):1-14.
- Kim KS. Bacterial meningitis beyond the neonatal period. [book auth.] Harrison GJ, Kaplan SL, et al Cherry JD. Feigin and Cherry's Textbook of Pediatric Infectious Diseases, 8th. Philadelphi : Elsevier, 2019, p. p.309.
- Lin TY, Nelson JD, McCracken GH Jr. Fever during treatment for bacterial meningitis. Pediatr Infect Dis. 1984;3(4):319-322. doi:10.1097/00006454-198407000-00009
- Kimberlin DW, Barnett ED, Lynfield R, et al. Report of the Committee on Infectious Diseases, 32nd ed. Itasca: American Academy of Pediatric, p.345., 2021.
- Oliveira CR, Morriss MC, Mistrot JG, et al. Brain magnetic resonance imaging of infants with bacterial meningitis [online]. J Pediatr. April 13, 2014. https://pubmed.ncbi.nlm.nih.gov/24726712/;165(1):134-139. doi:10.1016/j.jpeds.2014.02.061.
- Sheldon L, Kaplan MD. Bacterial meningitis in children: neurologic complications. [Online]. UpToDate. Jun 24, 2019. https://www-uptodate-com.db.rsu.lv/contents/bacterial-meningitis-in-children-neurologic-complications?search=haemophilus%20influenzae%20meningitis%20case%20report&topicRef=6010&source=see_link.
- Kornelisse RF, Westerbeek CM, Spoor AB, et al. Pneumococcal meningitis in children: prognostic indicators and outcome [online]. Clin Infect Dis. December 21, 1995. https://pubmed.ncbi.nlm.nih.gov/8749621/;21(6):1390-1397. doi:10.1093/clinids/21.6.1390.
|
| Correct Answers : |  100% 100% |
|
|
|
|
|
|