Sílvia Duarte Costa1, Sofia Silva Faria1, Cláudia Ferraz2, Ana Azevedo2.
1Department of Pediatrics, Unidade Local de Saúde de Matosinhos - Hospital Pedro Hispano, Porto, Portugal,
2Department of Neonatology, Unidade Local de Saúde de Matosinhos - Hospital Pedro Hispano, Porto, Portugal.
ADDRESS FOR CORRESPONDENCE
Sílvia Duarte Costa, Department of Pediatrics, Hospital Pedro Hispano, Rua Dr. Eduardo Torres, 4464-513 - Matosinhos, Portugal.
Email: silviagfdcosta@gmail.com | | Abstract | Background: Minimally/Less Invasive Surfactant Therapy/Administration (MIST/LISA) is increasingly used for surfactant delivery in preterm infants with respiratory distress syndrome (RDS), aiming to reduce complications associated with invasive methods. Despite its growing adoption, variations in clinical practice remain.
Objective: To evaluate MIST/LISA use in Portuguese neonatal intensive care units (NICUs) and identify variations in practice.
Methods: A national, anonymous questionnaire was distributed to neonatologists. The survey explored surfactant administration techniques, experience with MIST/LISA, device preferences, premedication strategies, and protocols. Responses were analyzed descriptively.
Results: Fifty-two responses were collected. Most respondents reported using MIST/LISA (87%), preferring it over INSURE or standard intubation. Practices varied widely in pre-intervention drugs use and catheter choice. Surfcath® was the most used device (71%). Only one-third consistently used pre-sedation.
Conclusion: MIST/LISA is widely implemented in Portuguese NICUs, but substantial variability exists. Standardized guidelines are needed to optimize clinical outcomes and reduce practice heterogeneity.
| | | | Keywords | | Surfactant Administration Techniques, Clinical Practice Variation, Respiratory Distress Syndrome, Neonatal Intensive Care Unit. | | | | Introduction | Respiratory distress syndrome (RDS) is a leading cause of morbidity and mortality in preterm infants, primarily due to pulmonary surfactant deficiency. Surfactant replacement therapy has significantly improved neonatal outcomes, traditionally administered via endotracheal intubation followed by mechanical ventilation. However, invasive ventilation is associated with complications such as bronchopulmonary dysplasia (BPD), volutrauma, and neurodevelopmental impairments.1,2 The Intubation-Surfactant-Extubation (INSURE) technique was introduced as a strategy to minimize the duration of mechanical ventilation by rapidly extubating the neonate after surfactant administration. Despite its benefits, INSURE still involves intubation, which carries procedural risks, including airway injury and hemodynamic instability.3,4 In response to these concerns, less invasive surfactant administration (LISA), also known as minimally invasive surfactant therapy (MIST), has gained attention as an alternative method. LISA allows surfactant to be delivered via a thin catheter while the neonate continues spontaneous breathing on nasal continuous positive airway pressure (nCPAP). Studies suggest that LISA reduces the need for mechanical ventilation, decreases BPD incidence, and improves overall respiratory outcomes.5,6 Despite its growing adoption, variations in LISA implementation persist across neonatal intensive care units (NICUs) around the world. Several randomized controlled trials (RCTs) and meta-analyses have compared LISA with INSURE, showing promising but sometimes inconclusive results regarding long-term benefits and optimal patient selection.2,3 Understanding the current practices and perceptions of LISA among neonatologists is crucial for optimizing its clinical application.
This study aims to evaluate the practice of MIST in neonatology, based on data from a national survey that investigates the implementation of this technique across various neonatal services. The findings will provide a comprehensive analysis of MIST’s application, helping to identify gaps in knowledge, clinical practices, and outcomes associated with this minimally invasive method.
| | | | Methods & Materials | | An anonymous questionnaire was sent to medical doctors working in neonatal intensive care units at a national level. It is important to note that the unit where each individual worked was never disclosed at any point in the questionnaire. The questionnaire was distributed via email to all units. The results were analyzed by two authors using the SPSS software. | | | | Results | Fifty two answers were received from professionals working in Neonatal Intensive Care Units (NICUs) in Portugal. All participants reported that they work in NICUs, and their years of experience in neonatology varied. Specifically, 14 respondents have more than 20 years of experience, ten have between 10 and 20 years, five have between 5 and 10 years, and ten have less than 5 years. This diversity reflects a broad range of professional experience among the respondents. There is an average of eight beds in the NICUs where the respondents work. In terms of the gestational age at which newborns are admitted to NICUs, 40 respondents said that their units admit neonates as early as 23/24 weeks gestation, three at 28 weeks, four at 30 weeks, two at 32 weeks, and three at 34 weeks. These results are described on the table A. This illustrates a degree of heterogeneity in procedures regarding the minimum gestational age for NICU admissions. Regarding the availability of protocols for surfactant administration, 33 respondents reported that their units have established protocols, while 19 reported that their units do not. When asked about their experience with the minimally invasive surfactant administration technique (MIST/LISA), 45 respondents stated that they had used it, while 7 did not. The MIST/LISA approach has been used in the participating NICUs for an average of six years.
Table 1.Presents respondent and unit characteristics, including professional experience, NICU capacity, gestational age admission criteria, and MIST/LISA technique usage.
| Years of experience |
- = > 20 years of experience: n=14 (26.9%)
- between 10 and 20 years: n=10 (19.2%)
- between 5 and 10 years: n=5 (9.6%)
- =5 years: n=10 (19.2%)
|
| Years of MIST/LISA technique usage (average) |
6 |
| Average number of beds |
8 |
| Minimum gestational age admitted |
=23/24 weeks gestation: n=40 (76.9%)
=28 weeks gestation: n=3 (5.8%)
=30 weeks gestation: n=4 (7.7%)
= 32 weeks gestation: n=2 (3.8%)
= 34 weeks gestation: n=3 (5.8%)
|
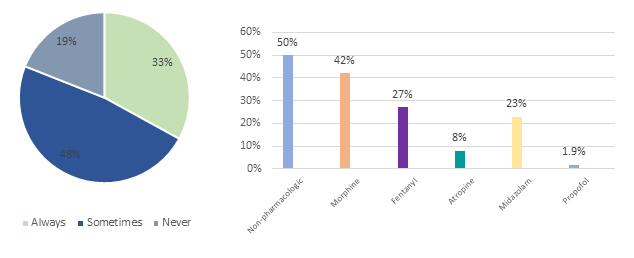
Concerning experience in surfactant delivery methods (Figure 1), 43 respondents reported applying standard intubation and mechanical ventilation, 44 using the INSURE technique (Intubation Surfactant Extubation), and 45 using the MIST/LISA approach. Notably, none of the respondents mentioned using pharyngeal or supraglottic administration to administer surfactant. 35 responders choose MIST/LISA for non-invasive ventilation of premature infants with Respiratory Distress Syndrome (RDS), 14 prefer INSURE, and 2 prefer conventional intubation. This highlights the growing demand for MIST/LISA in this therapeutic situation. When questioned about pre-treatment prescriptions before MIST/LISA, 48% (n=25) indicated that they sometimes provide medicines on the basis of individual circumstances, 33% (n=17) always use medication, and 19% (n=10) do not use any at all. In particular, 50% (n=26) of respondents reported utilizing nonpharmacological techniques, which were the most frequent approach in this group. morphine (42%), fentanyl (27%), atropine (8%), and midazolam (23%) were the most regularly utilized pre-treatment drugs, with one responder utilizing propofol (Figure 2).
Figure 1. Types of surfactant methods (n= absolute number of responses).
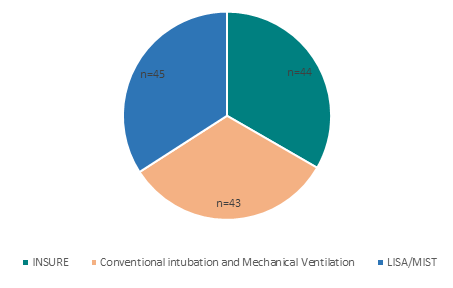
Figure 2. Premedication practices before MIST/LISA: frequency and types used.
Regarding the preferred devices for performing MIST, 37 respondents reported utilizing Surfcath®, a specialized catheter designed for MIST, whereas 7 use flexible catheters or gastric tubes, and one uses semi-rigid catheters (e.g., angiocaths). The remaining respondent did not use MIST. The most essential variables in selecting a device for MIST were catheter rigidity (63%), safety (58%), markings on the material (52%), less rigid tips (35%), design (27%), and pricing (9.6%).
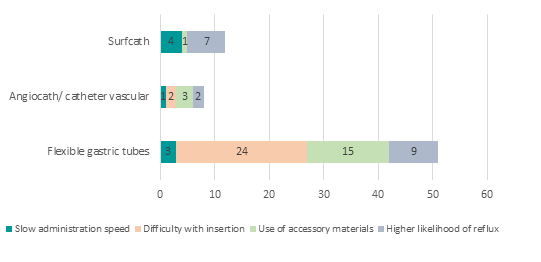
The strengths and limitations of various catheters used in MIST were also evaluated. Strengths for flexible gastric tubes were safety, whereas disadvantages included difficulty with insertion and slow administration of surfactant. Surfcath's strengths included rapid insertion, safety, ease of insertion, and procedural specificity, while its drawbacks included delayed administration and reflux. The angiocath/catheter vascular demonstrated few strengths, with only two respondents mentioning quick insertion and 13 respondents never using it (Figures 3 and 4). Umbilical catheters were described as having a limited function and were not preferred for MIST.
Figure 3. Absolute number of responses for each strength (advantage) associated with the different catheter types used in the MIST technique.
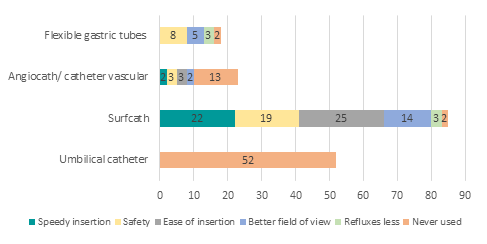
Figure 4. Absolute number of responses for each limitation associated with the different catheter types used in the MIST technique.
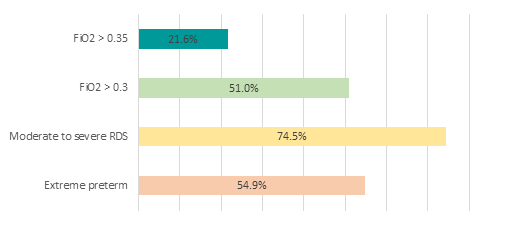
In terms of non-invasive administration with fine catheters, 52% reported using it for extremely premature infants, whereas 15% use it on delivery room stabilization. The most prevalent indications for initial surfactant administration were extreme preterm, moderate to severe RDS, FiO2 thresholds greater than 0.3, and FiO2 thresholds greater than 0.35 (Figure 5). The average first dose of surfactant used in participating NICUs was 200 mcg per kilo.
The most prevalent indication for the second dose of surfactant was increased respiratory distress (81%). The second dose was often given after 12 hours (65%), with a few providing it after 6 hours (19%) or 4 hours (3.8%).
Figure 5. Indications for initial surfactant administration.
Participants identified a number of challenges in surfactant administration by LISA, including difficulty intubating very premature infants, the need for laryngoscopy, limited resources for minimally invasive techniques, surfactant reflux, and procedure-related complications. Looking ahead, the most promising options for non-invasive surfactant delivery were nebulization (61%), the use of laryngeal masks (50%), novel catheters (26.9%), and videolaryngoscopy assistance (26.9%). | | | | Discussion | The results of this national survey illustrate a broad implementation of minimally invasive surfactant therapy (MIST/LISA) within NICUs, reflecting a progressive change in the management of respiratory distress syndrome (RDS) in infants born prematurely. A notable 87% of respondents reported using MIST, which is consistent with increasing research indicating that this technique lessens the reliance on invasive mechanical ventilation and its related complications, such as bronchopulmonary dysplasia (BPD), injuries to the lungs from ventilation, and neurodevelopmental challenges.1 These results are in agreement with prior randomized controlled trials (RCTs) and meta-analyses that have repeatedly shown that LISA leads to better respiratory outcomes and shorter ventilation periods compared to conventional intubation-surfactant-extubation (INSURE) or typical mechanical ventilation methods.2,7,8 However, despite favorable clinical uptake, a noticeable amount of procedural variation remains, especially regarding premedication practices and device selection, even with the favorable clinical uptake. Nearly half of the surveyed neonatologists reported either not using any sedation/analgesia before MIST or employing it selectively, which is consistent with the ongoing debate regarding the balance between procedural comfort and the risk of respiratory depression or hemodynamic instability induced by sedative agents.2,3,9 While morphine and fentanyl remain the most commonly used agents, their potential adverse effects emphasize the urgent need for standardized protocols or alternatives such as non-pharmacological interventions.1 More importantly, only half of the neonatologists reported utilizing nonpharmacological techniques, and that should be the subject of hard reflection as it is indicated in all the procedure protocols.
The preference for Surfcath® as the primary catheter for MIST administration was evident, valued for its rigidity, safety, and ease of insertion. Yet, a significant drawback identified was an increased incidence of surfactant reflux with Surfcath, which may reduce effective dosing and compromise clinical outcomes. This finding supports previous findings that catheter characteristics, such as tip rigidity and length, might affect surfactant delivery efficiency and reflux rates.1,5,10 On the other hand, flexible catheters appeared to reduce reflux despite being slower for surfactant instillation and more challenging to insert. This suggests a trade-off between therapeutic efficacy and ease of use that deserves more comparative research. The study also highlights that MIST is primarily employed in extremely premature infants with moderate to severe RDS, often guided by oxygen requirements (FiO2 >0.3), reflecting adherence to evidence-based criteria for surfactant administration, in accordance with European guidelines.5,6 The reported average initial surfactant dose of 200 mcg/kg aligns with established dosing recommendations and is consistent with protocols used in recent clinical trials, reinforcing the clinical relevance of the surveyed practices.1,4 Respondent-identified difficulties with laryngoscopy of extremely preterm newborns, limited institutional resources, surfactant reflux, and procedural problems highlight areas that require training and quality improvement. Innovations including nebulized surfactant delivery, laryngeal mask airways, and videolaryngoscopy are promising approaches to improving the safety and effectiveness of non-invasive surfactant administration and should be further studied.1,4 | | | | Conclusion | | This national survey highlights the widespread use of MIST/LISA in Portuguese NICUs while revealing important variability in its clinical application, particularly regarding pre-intervention drugs and device choice. These findings underscore the need for clearer protocols and may support future efforts toward practice standardization. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Mani S, Rawat M. Less Invasive Surfactant Administration: A Viewpoint. Am J Perinatol. 2024;41:211-227. [CrossRef] [PubMed] [PMC free article]
- Kuitunen I, Räsänen K. Less Invasive Surfactant Administration Compared to Intubation, Surfactant, Rapid Extubation Method in Preterm Neonates: An Umbrella Review. Neonatology. 2024;121:485-493. [CrossRef] [PubMed] [PMC free article]
- Dini G, Santini MG, Celi F, Verrotti A. Less invasive surfactant administration versus intubation-surfactant-extubation in preterm infants: a retrospective study. Med Glas (Zenica). 2024;21(2). [CrossRef] [PubMed]
- Kim SY, Lim J, Shim GH. Comparison of mortality and short-term outcomes between classic, intubation-surfactant-extubation, and less invasive surfactant administration methods of surfactant replacement therapy. Front Pediatr. 2023;11:1197607. [CrossRef] [PubMed] [PMC free article]
- Silveira RC, Panceri C, Munõz NP, et al. Less invasive surfactant administration versus intubation-surfactant-extubation in the treatment of neonatal respiratory distress syndrome: a systematic review and meta-analyses. Jornal de Pediatria. 2024;100(1):8-24 [CrossRef] [PubMed] [PMC free article]
- Sweet DG, et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2022 Update. Neonatology. 2023;120(3):1-23. [CrossRef] [PubMed] [PMC free article]
- Kribs A, et al. Nonintubated surfactant application vs conventional therapy in extremely preterm infants: A randomized clinical trial (AMV study). JAMA Pediatr. 2015;169(8):723-730. [CrossRef] [PubMed]
- Zhou K, et al. Comparison of Less Invasive Surfactant Administration With Intubation-Surfactant-Extubation in Very Preterm Infants: A Meta-analysis. JAMA Pediatr. 2021;175(9):e211847.
- Brüesch T, et al. Premedication for less invasive surfactant administration (LISA) in neonates: a systematic review. Arch Dis Child Fetal Neonatal Ed. 2021;106(6):659-665.
- Dargaville PA, et al. Minimally invasive surfactant therapy: an updated review. Pediatr Res. 2021;90(5):732-740.
DOI: https://doi.org/10.7199/ped.oncall.2027.5
|
| Cite this article as: | | Costa S D, Faria S S, Ferraz C, Azevedo A. MIST/LISA in Portugal: National Survey of Clinical Practice. Pediatr Oncall J. 2026 Feb 27. doi: 10.7199/ped.oncall.2027.5 |
|