Sanghamitra Ray, Prakash Chand Jain.
Department of pediatrics, Cantonment General Hospital, Delhi Cantt, New Delhi.
ADDRESS FOR CORRESPONDENCE
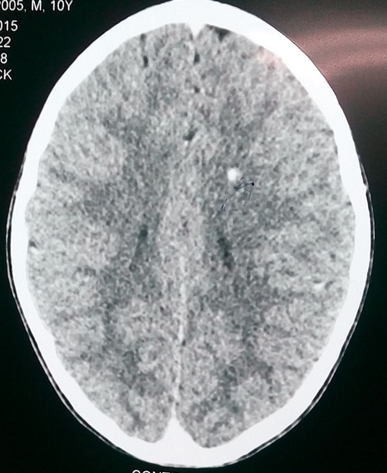
Dr Sanghamitra Ray, (M.D. Pediatrics), Flat No- 176, Pocket-1, Sector-1, Dwarka. New Delhi 110075. India. | | Keywords | | Cysticercosis cutis, Neurocysticercosis | | | A 10 years old girl presented with a small swelling over left cheek of 5 years duration. Swelling was skin-colored, well-circumscribed, non-tender, firm, mobile and size 4 X 4 cm in diameter. The swelling was not very obvious on inspection. There was no regional or generalized lymphadenopathy. Systemic examination was normal. Initially she received antibiotic course for the swelling before coming to us. Fine needle aspiration cytology (FNAC) was suggestive of subcutaneous cysticercosis with documentation of tegument layer, fibro-collagenous tissue and chronic inflammatory cells consisting of eosinophil, lymphocyte and plasma cells. On further inquiry, she informed that she used to eat non-vegetarian food occasionally. Ophthalmological examination was normal. There were no other swellings elsewhere in the body. Contrast-enhanced computed tomography (CECT) scan of brain revealed a small calcified granuloma in the left parietal lobe with no perilesional edema. (Figure 1) Ultrasound abdomen was normal. There was no eosinophilia on hemogram. Stool microscopy was also unremarkable. She was given albendazole (15 mg/kg/day) for 28 days. All other family members were given a single dose of albendazole as prophylaxis measure along with hygiene education. On follow up the swelling reduced in size and no neurological symptom was detected. Repeat neuroimaging was not done.
Figure. 1 CECT Brain showing calcified granuloma in left parietal lobe
Neurocysticercosis is a major cause of neurologic disease worldwide. The clinical presentations are pleomorphic depending on the stage and location of cysts. Most children (> 80%) present with seizures; headache and vomiting are seen in about a third of cases. (1) Approximately half of the patients with cysticercosis present with subcutaneous nodules. (2) However, the association of neural and subcutaneous cysticercosis is not common and very few cases have been reported in literature. (3-5) They may be confused with other painless swellings such as lymphadenopathies, neurofibromas, and epidermoid cysts. In a developing country like India, a rapid, safe and reliable cytological diagnosis of subcutaneous cysticercosis by FNAC on an outpatient basis proves to be cost-effective. (6)
The management of cysticercosis involve antihelminthics and in some situations steroids to reduce inflammation if present. Individual subcutaneous cysts may be removed if desired. Seizures very commonly occur in the presence of calcified granulomas; moreover recurrent, episodes of perilesional edema maximally centered around the calcifications have also been described leading to refractory seizures. Therefore, calcified granuloma if associated with other evidence of active cysticercosis should be treated.
This case highlights the need to evaluate even so called dormant swellings of long duration and to reach a tissue diagnosis. This patient unless worked up properly, CNS granuloma would have been missed and she could have manifested with seizure as most cases of neurocysticercosis.
| | | | Contributor Statement | | SR and PCJ both were involved in the case management. SR did the literature search and drafting of the manuscript. PCJ reviewed the final drafting and supervised. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Singhi P, Singhi S. Neurocysticercosis in children. Child Neurol. 2004 Jul;19(7):482-92. [CrossRef] [PubMed]
- Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ. Fitzpatrick's Dermatology in General Medicine. 7th ed. USA. The McGraw Hill Companies Inc. 2008. pp. 2027–8.
- Singrodia S, Joshi RG, Solanki RB, Rawal RC. Subcutaneous nodules preceding convulsions due to neural cysticercosis. Indian J Dermatol Venereol Leprol. 2008;74:385–6. [CrossRef] [PubMed]
- Gupta S, Jain VK, Sen J, Gupta S, Arora B. Subcutaneous cysticercosis involving the eyelid: sonographic diagnosis. J Dermatol. 2000;27(1):35-9. [CrossRef] [PubMed]
- Uthida-Tanaka AM, Sampaio MC, Velho PE, Damasceno BP, Cintra ML, de Moraes AM, Zanardi V. Subcutaneous and cerebral cysticercosis. J Am Acad Dermatol. 2004;50(2 Suppl):S14-7. [CrossRef]
- Kamal MM, Grover SV. Cytomorphology of subcutaneous cysticercosis. A report of 10 cases. Acta Cytol. 1995 Jul-Aug; 39(4):809-12. [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2016.10
|
| Cite this article as: | | Ray S, Jain P C. Cysticercosis Cutis- An Unusual Guide to Neurocysticercosis. Pediatr Oncall J. 2016;13: 25. doi: 10.7199/ped.oncall.2016.10 |
|