Sharad Agarkhedkar, Geeta Karambelkar, Shraddha Salunkhe, Bonny Baracho.
Department of Pediatrics, Dr D Y Patil Medical College, Pune, Maharashtra, India.
ADDRESS FOR CORRESPONDENCE
Dr Bonny Baracho, Flat number 102, Building name Sheldon F1, Sukhwani Campus, Opposite ST Bus Stand, Vallabh Nagar, Pimpri, Pune, Maharashtra 411018.
Email: bonnybaracho22@gmail.com | A seven-months-old male, first born of a non-consanguineous marriage, presented with repeated tonic clonic convulsions since three months of age and recurrent respiratory infections since four months of age. He had delayed development and had still not achieved head holding or social smile. On examination, weight was 6.9 kgs, length was 68 cms, head circumference was 40 cms, there was pallor, he had fair complexion and light coloured steel sparse woolly hair with easy pluckability. On systemic examination, he had brisk deep tendon reflexes and hypotonia. Other systems were normal. On investigations, serum copper was 6.47mcg/dl (normal= 90-190 mcg/dl), serum ceruloplasmin level was 3.94 mg/dl (normal = 20-60 mg/dl). MRI brain showed altered signal intensity diffusely involving the periventricular white matter and cortex in bilateral cerebral hemispheres with gross thinning of cortex. MR angiography revealed tortuosity of cerebral vessels (Figure 1). EEG showed left temporo-occipital epileptiform activity. Microscopic examination of hair revealed classical sign of pili torti. The child was treated symptomatically with anticonvulsant drugs and discharged.
Fig 1: MR angiography showing tortuosity of cerebral vessels.
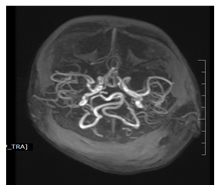
Menkes disease is an X-linked lethal multi-system disorder caused by disturbances of copper distribution in different tissues due to mutation of ATPase 7a gene. The estimated incidence of the disease is 1 in 1,00,000 to1 in 2,50,000. (1) The affected individual suffers from malfunction of copper containing enzymes resulting in multi-systemic disturbances. Nervous system problems include gross mental retardation, convulsions, cortical atrophy, asymptomatic subdural effusion, gross truncal hypotonia and progressive neurological deterioration. Vascular problems with weak collagen tissues cause easy breakability, connective tissue abnormality gives rise to characteristics steel, fuzzy, woolly, sparse hair with easy pluckability. (2) There are chances of recurrent infections and as a result the infant fails to thrive and malnutrition is a common finding. (3) Children usually die within 3–4 years of age. (4) Clinical history and the appearance of the infant should suggest the diagnosis. Microscopic examination of hair reveals classical pili torti. Normally, in healthy children, concentrations of plasma copper and ceruloplasmin tend to be low during the first 3 weeks of life, may decrease even after the 6th week of life, and can sometimes be low even up to 6 months of age. In Menkes disease, serum copper and ceruloplasmin continue to remain low. MRI brain in Menkes disease shows tortuosity of cerebral vessels. (5) Our patient also had woolly hair, pili torti on microscopy, low serum copper and ceruloplasmin and MRI brain showed tortuosity of cerebral vessels.
There is no cure for Menkes disease. Early treatment with subcutaneous, intramuscular, or intravenous injections of copper supplements (in the form of acetate salts) may be of some benefit. (6) Other treatment is symptomatic and supportive. The prognosis of this disease is poor because currently there is no effective way to detect the disorder early in newborns, therefore many individuals die within the first few years of life. (7) | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Kirodian BG, Gogtay NJ, Udani VP, Kshirsagar NA. Treatment of Menkes disease with parental copper histidine. Indian Pediatrics. 2002;39:183–185. [PubMed]
- Danks DM, Campbell PE, Stevens BJ, Mayne V, Cartwright E. Menkes kinkey hair syndrome An Inherited defect of copper absorption with widespread effects. Pediatrics. 1972;50:188–201. [PubMed]
- Kodama H, Murata Y, Kabayashi M. Clinical manifestations and treatment of Menkes disease and its variants. Pediatr Int. 1999; 41:423–429. [CrossRef] [PubMed]
- Drank DM, Cartwright E, Stevens BJ, Townley RR. Menkes kinkey hair disease: Further definition of the defect in copper transport. Science. 1973;1:1140–2.
- Christodoulou J, Danks DM, Sarkar B, Baerlocher KE, Casey R, Horn N, et al. Early treatment of Menkes disease with parenteral copper-histidine: long-term follow-up of four treated patients. Am J Med Jenet. 1998;76:154–164. [CrossRef]
- Mollar LB, Tumer Z, Lund C, Petersen C, Cole T, Hanusch R et al. Similar splice site mutations of ATP7A gene lead to different phenotypes: classical Menkes disease or occipital horn syndrome. Am J Human Genet. 2000;66:1211–20. [CrossRef] [PubMed] [PMC free article]
- Kaler SG, Holmes CS, Goldstein DS, Tang J, Godwin SC, Donsante A, et al. Neonatal diagnosis and treatment of Menkes disease. N Engl J Med. 2008;358:605-14. [CrossRef] [PubMed] [PMC free article]
DOI: https://doi.org/10.7199/ped.oncall.2016.34
|
| Cite this article as: | | Agarkhedkar S, Karambelkar G, Salunkhe S, Baracho B. Menkes Disease. Pediatr Oncall J. 2016;13: 77. doi: 10.7199/ped.oncall.2016.34 |
|