Nonyelum Ebigbo, Anthony Barone, Santosh Parab.
Department of Pediatrics, Richmond University Medical Center, Staten Island, New York, USA.
ADDRESS FOR CORRESPONDENCE
Santosh Parab, Department of Pediatrics, Richmond University Medical Center, 355 Bard Avenue, Staten Island, New York 10310, USA.
Email: sparab@rumcsi.org | | Abstract | | A preterm female neonate born at 30 weeks gestation was noted to have abdominal calcification on routine radiograph of the chest/abdomen. Patient developed intermittent abdominal distension and feeding intolerance. Barium enema revealed a stricture in the transverse colon. Patient underwent an exploratory laparotomy which revealed a colonic stricture with walled off adhesions indicative of in-utero perforation. Histology confirmed a diagnosis of meconium peritonitis. | | | | Keywords | | Meconium Peritonitis, Calcification | | | | Introduction | The presence of intra-abdominal calcification in an otherwise asymptomatic neonate can be a presenting feature of neuroblastoma, fetus-in-fetu, meconium peritonitis, hepatic calcifications following intra-uterine fetal congenital infections, parvovirus B19 infection and vascular pathology such as hemangiomas. (1)
Meconium peritonitis is a rare condition with a reported frequency of 1:35000 neonates. (1,2) It is secondary to antenatal perforation owing to intestinal ischemia, with or without bowel obstruction (due to volvulus, stenosis, atresia, intussusception, congenital bands, Meckel diverticulum and internal hernia), viral infections and inspissation of abnormal meconium (as in cystic fibrosis). Meconium ileus accounts for less than 25% of cases of meconium peritonitis. (3) Various studies have also described an association with maternal liver disease. (4)
We present a preterm neonate who had abdominal calcification at birth. Barium enema revealed a stricture in the transverse colon. Exploratory laparotomy revealed a colonic stricture with walled off perforation and adhesions. Histology confirmed a diagnosis of meconium peritonitis. | | | | Case Report | A female neonate with birthweight of 1729g was delivered vaginally at 30 weeks gestational age to an 18-year-old G2P1 mother due to preterm labor. Antenatal course was only significant for cervical cerclage for cervical incompetence. Mother received antenatal course of steroids and magnesium sulfate. Baby had APGAR scores of 8 and 9 at 1 and 5 minutes respectively. After admission to Neonatal Intensive Care Unit (NICU), baby was placed on nasal Continuous Positive Airway Pressure (CPAP) for mild Respiratory Distress Syndrome (RDS). Right upper quadrant calcification was noted on initial Chest X-ray (Fig 1). On abdominal ultrasound, the calcification was initially thought to be a hepatic subcapsular calcification. Test for TORCH infections was negative. As per New York State protocol, newborn screen for predominant metabolic and genetic diseases was negative. Liver function tests were normal. Head ultrasound was normal. The placental histopathology was unremarkable. Baby was started on feeds on the third day of life and progressed gradually. She had intermittent bouts of abdominal distension and feeding intolerance, but was able to progress to full enteral feeds by the twelfth day of life. The calcification remained the same on subsequent radiographs. A barium enema done on the 34th day of life in view of intermittent abdominal distension showed persistent narrowing at the right transverse colon with a dilated cecum and a collapse of the colon distal to the narrowing. (Fig 2). Barium was visualized passing through the strictured site and into the ascending colon. The calcification seen initially was noted to be extra-luminal. Exploratory laparotomy for correcting the stricture revealed a dilated proximal colon with dense adhesions and calcification in the region of the gall bladder with internal bowel herniation. There was also a walled off perforation with adhesions at the level of the ileum about 15cm from the ileocecal junction and dilation of the small bowel proximally. Adhesiolysis, excision of hernia and transverse strictureplasty was done. Histology of excised mass showed fragments of calcified amorphous material, chronic inflammation and pigmented histiocytes compatible with meconium peritonitis. (Fig 3). She did well after surgery, resumed normal feedings on 7th post-op day and was discharged home on day 48 of life.
Fig 1: Arrow showing right upper quadrant calcification

Fig 2: Barium enema showing narrowing of the right transverse colon

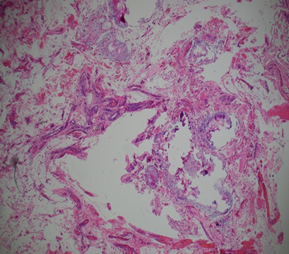
Fig 3: Fragments of amorphous calcified material. Magnification: 10X
 | | | | Discussion | Meconium is a sterile mixture of swallowed amniotic fluid, bile salts, bile pigments, cholesterol, mucin, pancreatic enzymes, and intestinal enzymes. Extrusion of meconium with intestinal necrosis can cause inflammatory reaction leading to calcification of cornified epithelial cells which are part of the extravasated meconium and extensive scarring. This perforation usually occurs proximal to an obstruction. The most common site of perforation is the small bowel, the distal ileum being the most frequent site. (5) The exact cause of obstruction in the transverse colon in our case is not known. Calcification from meconium peritonitis is usually intraperitoneal, some reports have described scrotal and thoracic extensions. (6,7)
Meconium peritonitis has four clinical variants: 1) fibro-adhesive meconium peritonitis where extensive scarring seals the perforation, as in this patient; 2) cystic meconium peritonitis results if meconium continues to leak into peritoneal cavity, causing formation of a cyst; 3) meconium pseudocyst where loops of bowel and necrotic tissue are encased in scar tissue and surround the extra mural meconium; and, 4) meconium ascites where perforation occurs just before delivery accompanied by exudative leak into the abdominal cavity. (8)
Radiographic differentiation of meconium peritonitis from other causes of intraabdominal calcification is often possible and fetal ultrasound may also provide important clues to the diagnosis. (1) Up to 86% of cases of meconium peritonitis may have intraabdominal calcifications which may be detected as early as 18-week gestational age. These calcifications are usually characteristic and usually appear as linear or plaque-like lesions in the pelvis, peritoneum, scrotum and may even appear in the undersurface of the liver. (3). Other ultrasound findings include fetal ascites, dilated bowel loops, pseudocysts and/or polyhydramnios. (5) In a study by Tsai et al (9), ascites was the most common finding on prenatal ultrasound. It has been hypothesized that perforated intestines can heal spontaneously in utero if the prenatal period is long enough. Fetal ascites, polyhydramnios and dilated bowel loops can resolve spontaneously during the prenatal period, usually after the intestine heals. (1) Radiological investigations including plain radiograph, ultrasound and water-soluble contrast studies may be required to establish the diagnosis postnatally.
Neonatal outcomes are much better if detected prenatally than if diagnosed after birth. (2) Early detection of meconium peritonitis is not indicative of poor neonatal outcomes. Resolution of dilated bowel loops and polyhydramnios are related to low rates of postnatal surgery. The pseudocyst variant is associated with poor outcome. (3)
High mortality had been previously reported, though recent studies reported higher survival rates if diagnosis was made using prenatal ultrasound. (10) Mortality is reported in 10 to 50% of the cases with in utero bowel perforation needing post-surgical intervention. (1,5) Overall survival rate in recent studies is around 85-92%. (1,8) | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Wang C, Wang T, Chang Y, Chang S, Chao A, Tseng L. Meconium Peritonitis In Utero—the Value of Prenatal Diagnosis in Determining Neonatal Outcome. Taiwan J Obstet Gynecol. 2008 Dec;47(4):391-6. [CrossRef]
- Sharma D, Murki S, Pratap T. Meconium peritonitis: an interesting entity. BMJ Case Rep. 2014 May 5;2014. pii: bcr2014203536.
- Park RW, Grand RJ. Gastrointestinal Manifestation of Cystic Fibrosis: A Review. Gastroenterology. 1981 Dec;81(6):1143-61.
- Lai CWS, Shek NWM. Fetal Meconium Peritonitis and Maternal Liver Disease. Obstet Gynecol. 2016 Apr;127(4):740-3. [CrossRef]
- Rajendra KG, Jyoti S. In utero Intestinal Perforation presenting as ileal atresia with calcification: A case report. J Clin Diagn Res. 2011; 5(2):347-349.
- Kimball D, Smith W. Meconium peritonitis with thoracic extension. Am J Roentgenol. 1985 Jan;144(1):113-4. [CrossRef] [PubMed]
- Berdon WE, Baker J, DeSanctis P. Scrotal masses in healed meconium peritonitis. N Engl J Med 1967;227:585-587. [CrossRef]
- Nam SH, Kim AR, Kim SC, Kim DY, Kim KS, Pi SY, et al. Experience with meconium peritonitis. J Pediatr Surg. 2007;42:1822-1825. [CrossRef]
- Tsai M, Chu S, Lien R, Huang H, Luo C. Clinical Manifestations in Infants with Symptomatic Meconium Peritonitis. Pediatr-Neonatol. 2009;50:59-64. [CrossRef]
- Tibboel D, Gaillard JL, Molenaar JC. The importance of mesenteric vascular insufficiency in meconium peritonitis. Hum Pathol. 1986 Apr;17(4):411-6. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2017.46
|
| Cite this article as: | | Ebigbo N, Barone A, Parab S. Abdominal Calcification - Is it Meconium Peritonitis?. Pediatr Oncall J. 2017;14: 90-91. doi: 10.7199/ped.oncall.2017.46 |
|