|
Fever, Headache and Raised Intracranial Pressure
Anjali Bharani, Pramila Ramawat, Swati Raipurkar.
Department of Pediatrics, Index Medical College, Hospital and Research Centre, Indore, Madhya Pradesh, India.
ADDRESS FOR CORRESPONDENCE
Dr Anjali Bharani, 119, Ravindra Nagar, Indore 452018, Madhya Pradesh, India.
Email: dr.anjalibharani@gmail.com

|

|
What is the diagnosis and how to treat it?
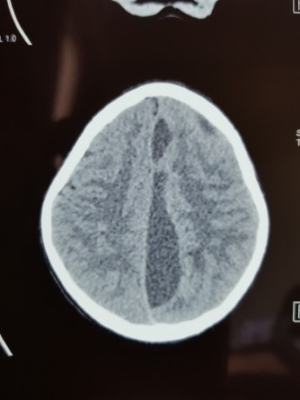
CECT showed a large (11.15 x 2.4) left sided parafalcine subdural empyema with cerebritis and uncal herniation and shift of midline with features of raised intracranial tension. Parafalcine and subdural empyemas generally are life-threatening diseases that require an emergent treatment. (1) They can be caused by trauma, neurosurgical procedures, hematogenous (2) and contiguous spreading of an infection. (3) The contiguous spread in children and adolescents can arise as extensions from both otologic and paranasal sinus disease. (4) The symptoms of parafalcine empyemas can vary from unspecific symptoms like fever and headache to neurological symptoms like hemiparesis, impairment of consciousness until seizures. Left untreated infection may spread intracranially and lead to increased morbidity and mortality. Subdural empyemas, in particular, may lead to cortical venous thrombosis and potentially devastating venous congestion and infarction. If not detected and treated early, it may reach giant size. (5) Prompt treatment with intravenous broad spectrum antibiotics and craniotomy and surgical evacuation of pus by craniotomy and if, necessary anti-epileptic therapy improves outcomes in such patients. Some of these patients are known to require repeat surgical evacuation in view of recurrence of symptoms and abscess on imaging during follow-up. (6)
Our patient was started on intravenous ceftriaxone, vancomycin and metronidazole. Neurosurgeons advised craniotomy and evacuation of the pus, but parents took her home against medical advice. |
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
|
- Banerjee AD, Pandey P, Devi BI, Sampath S, Chandramouli BA, et al. Pediatric supratentorial subdural empyemas: a retrospective analysis of 65 cases. Pediatr Neurosurg. 2009;45:11–8. [CrossRef] [PubMed]
- Salunke PS, Malik V, Kovai P, Mukherjee KK. Falcotentorial subdural empyema: analysis of 10 cases. Acta Neurochir (Wien) 2011;153:164–9. [CrossRef] [PubMed]
- Ak HE, Ozkan U, Devecioglu C, Kemaloglu MS. Treatment of subdural empyema by burr hole. Isr J Med Sci. 1996;32:542–4. [PubMed]
- Mueller K, Myseros J. Pediatric Intrafalcine Empyema from a Sinogenic Origin: A Case Report. Cureus. 2017; 9(5): e1223. [CrossRef]
- Hicdonmez T, Cakir B, Hamamcioglu MK, Kilincer C, Cobanoglu S. Giant subdural empyema in a child: a case report. Surgical Neurology. 2006; 66: 632–633. [CrossRef] [PubMed]
- Niklewski F, Petridis AK, JA, Blaeser K, Ntoulias G, Bitter A, Rosenbaum T, Scholz M. Pediatric parafalcine empyemas. J Surg Case Rep.2013; 8: rjt067.
|
|
DOI: https://doi.org/10.7199/ped.oncall.2018.36 |
| |
Cite this article as:
Bharani A, Ramawat P, Raipurkar S. Fever, Headache and Raised Intracranial Pressure. Pediatr Oncall J. 2018;15: 82. doi: 10.7199/ped.oncall.2018.36
|