Acute encephalopathy: What to suspect and how to prevent?
|
|
Acute encephalopathy: What to suspect and how to prevent?
20/02/2021
20/02/2021
https://www.pediatriconcall.com/Journal/images/journal_cover.jpg
Vinod Kumar Gupta1, Vanita Verma2, RK Yadav1, Mukesh Vir Singh1, Anubha Shrivastava1.
1Department of Pediatrics, MLN Medical College, Prayagraj, Uttar Pradesh, India,
2National Diagnostics, New Delhi, India.
ADDRESS FOR CORRESPONDENCE
Dr. Anubha Shrivastava, 84, Lukerganj, Prayagraj, Uttar Pradesh 211016, India.
Email: anubhashrivastava@rediffmail.com
acute necrotizing encephalopathy, childhood
|
Clinical Problem
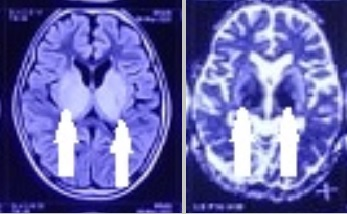
A 9-year-old girl presented with convulsions followed by unconsciousness. She had fever and cough for one week. On examination, Glasgow coma score (GCS) was 8/15. There were no meningeal signs or focal weakness. Fundus examination was normal. Other systemic examination was normal. Investigations showed hemoglobin 11 g/dl, total leucocyte count 4200/cumm with 52% polymorphs and 39% lymphocytes, serum bilirubin 0.5 mg/dL with normal transaminases and INR of 1.9. Arterial blood gas showed pH of 7.38 and bicarbonate 23 mEq/L. Lumbar puncture showed clear cerebrospinal fluid (CSF) with normal pressure, 71.4 mg/dL glucose, 16.2 mg/dL protein, 4 cells/cumm (mostly polymorphs and few degenerated cells) and no bacteria. Nasopharyngeal swab was negative for Covid-19 RT-PCR. Blood and CSF was negative for Japanese Encephalitis IgM. Testing for influenza virus was unavailable at our centre. MRI brain showed symmetrical hyper-intense signal intensity on T2W/FLAIR, restricted diffusion on DWI and signal drop (apparent diffusion coefficient) involving bilateral ganglio-thalamic complexes, brain stem and cerebral peduncles (Figure 1). Injection ceftriaxone (100 mg/kg/day in 2 divided doses), vancomycin (60 mg/kg/day in 4 divided doses) and acyclovir (45 mg/kg/day in 3 divided doses) were started intravenously (IV). Oseltamivir was unavailable. Convulsions were controlled with levericetam (40 mg/kg/day in 2 divided doses). Intravenous Immunoglobulin (IVIG) (30mg/kg/day for 3 days) followed by oral prednisolone (2 mg/kg/day in 2 divided doses) were also given. On 3rd day, patient showed improved sensorium and no further convulsions. On follow-up at three months, distal athetoid movements remained but repeat MRI brain showed resolution.
|
Figure 1. MRI brain shows thalamic hyperintensity on T2W and restricted diffusion in bilateral thalamus on DWI.
|
| |
What is the diagnosis?
|
|
|
Discussion
Acute necrotising encephalopathy of childhood (ANEC). Mizuguchi et al described ANEC in Japan in 1995.1 Most cases are from East Asia but not limited to any particular race.2 ANEC follows infection with influenza, Herpes Simplex Virus, Human Herpes Virus-6, Parainfluenza virus, Varicella Zoster Virus, reovirus, rotavirus, enterovirus, measles, coxsackie-A9 and mycoplasma.3 ANEC occurs within days of fever and presents with convulsions and coma.1 Acute manifestations are febrile seizures, movement disorder, frontal lobe encephalopathy and multiorgan failure.2,3 Subacute manifestations are Guillain-Barre syndrome, transverse myelitis, acute disseminated encephalomyelitis, cerebellitis and myositis. Late manifestations are parkinsonism and encephalitis lethargica.3 Patients of 2009 H1N1 influenza pandemic showed heightened neurological complications and ANEC compared to 2004–2008 seasonal influenza.3 Cytokine storm following viral infection leads to systemic immune response causing multiorgan injury, brain cell apoptosis and cerebral edema from disruption of blood-brain barrier in ANEC.2,3 RANBP2 genetic polymorphism is associated with recurrent episodes of ANEC with viral respiratory infections.4 Central necrosis, surrounding cytotoxic oedema and peripheral vasogenic oedema forms pathological basis for MRI appearance.3 T1W show hypointense lesions, T2W/FLAIR display corresponding mixed hyperintense signals with restricted diffusion on DWI and circular enhancement on contrast MRI.2 Normal CSF and characteristic bilateral thalamic involvement with diffusion restriction help in making diagnosis.5 Acute disseminated encephalomyelitis, neurovascular accidents, Reye’s syndrome, mitochondrial dysfunction and fulminant hepatitis are other differentials.3,6 Outcomes range from full recovery (<10%), neurologic sequelae in survivors to fulminant progression in majority.3 Li et al observed positive correlation between MRI findings and clinical outcome.2 Observation of hemorrhage and local tissue loss on MRI predicts a poor prognosis.2 Selective vulnerability of thalami seems to be determining factor.6 Antivirals, immunoglobulin, plasmapheresis, antithrombin-III, and therapeutic hypothermia has been tried.3 High dose steroids used in earlier stages determines the prognosis.6 Follow-up imaging shows regression of lesions with residual cortical atrophy, cystic changes and haemosiderin deposition. Functional recovery following rehabilitation has been reported.3
Given the potential for ANEC recurrence, monitoring of children with history of neurological complications following respiratory illness is indicated during influenza season with prompt testing and antiviral therapy.4 Annual influenza vaccination is important for ANEC survivors and their household contacts.4
|
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
- Mizuguchi M, Abe J, Mikkaichi K, Noma S, Yoshida K, Yamanaka T, Kamoshita S. Acute necrotising encephalopathy of childhood: a new syndrome presenting with multifocal, symmetric brain lesions. J Neurol Neurosurg Psychiatry. 1995;58:555-561. [CrossRef] [PubMed] [PMC free article]
- Li H, Sun C, Chi S, Wang Y, Wu L, Qin X. Use of MRI in the diagnosis and prognosis of acute necrotizing encephalopathy in a Chinese teenager. Medicine 2019;98:44. [CrossRef] [PubMed] [PMC free article]
- Yoganathan S, Sudhakar SV, James EJ, Thomas MM. Acute necrotising encephalopathy in a child with H1N1 influenza infection: a clinicoradiological diagnosis and follow-up. BMJ Case Rep. 2016 Jan 11;2016:bcr2015213429. [CrossRef] [PubMed] [PMC free article]
- Howard A, Uyeki TM, Fergie J. Influenza-Associated Acute Necrotizing Encephalopathy in Siblings. J Pediatric Infect Dis Soc. 2018;7: e172-177. [CrossRef] [PubMed] [PMC free article]
- Sharma M, Sood D, Chauhan NS, Negi P. Acute necrotizing encephalopathy of childhood. Neurol India. 2019;67:610‐611. [CrossRef] [PubMed]
- Seo HE, Hwang SK, Choe BH, Cho MH, Park SP, Kwon S. Clinical spectrum and prognostic factors of acute necrotizing encephalopathy in children. J Korean Med Sci. 2010;25:449-453. [CrossRef] [PubMed] [PMC free article]
|
|
| |
Cite this article as:
Gupta V K, Verma V, Yadav R, Singh M V, Shrivastava A. Acute encephalopathy: What to suspect and how to prevent?. Pediatr Oncall J. 2021;18: 30-31. doi: 10.7199/ped.oncall.2021.12
|