Knocking Down the Diagnosis in Knock Knees
|
|
Knocking Down the Diagnosis in Knock Knees
27/04/2021
27/04/2021
https://www.pediatriconcall.com/Journal/images/journal_cover.jpg
Anilkumar M Khamkar1, Georgeena Elsa Jose2, P D Pote2, Pradeep Suryawanshi1.
1Department of Neonatology, Noble Hospital and Research Center, Pune, Maharashtra, India,
2Department of Pediatrics, Noble Hospital and Research Center, Pune, Maharashtra, India.
ADDRESS FOR CORRESPONDENCE
Dr. Georgeena Elsa Jose, Junior Resident -1, Department of Pediatrics, Noble Hospital and Research Center, 153, Magarpatta City Road, Pune, India - 411013.
Email: egeorgeena@gmail.com
Bardet-Biedl Syndrome, Knock Knees, Obesity, Polydactyly, Retinitis pigmentosa
|
Clinical Problem
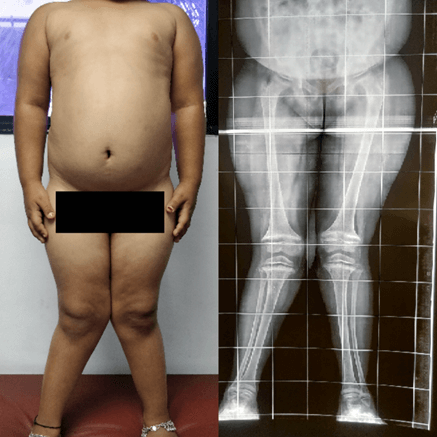
An 8-year-old girl, born of 2nd degree consanguineous marriage presented with bilateral lower limb deformity and not gaining height. Other problems included poor scholastic performance, diminished vision in both eyes especially at night and excessive weight gain from 2 years of age. She was operated for left sided complete cleft lip and palate at 3 years of age (Figure 1). She also had delayed developmental milestones, with commencement of walking and speech at 2 and 5 years of age, respectively. On examination, bilateral genu valgum (inter-malleolar distance was 20 cm) and post-axial hexadactyly and brachydactyly of all four limbs were seen (Figure 2). Her height was below 3rd percentile and her weight was at 25th percentile according to the Indian Academy of Pediatrics (IAP) charts, with a body mass index (BMI) above 97th percentile according to the World Health Organization (WHO) criteria. She had a waist to hip ratio of 0.89, fitting into central obesity. She also had Stage 2 hypertension [blood pressure (BP) 132/90 mm of Hg]. Ophthalmic examination revealed myopic astigmatism along with retinitis pigmentosa. Among the laboratory investigations (Table 1), she had severe Vitamin D deficiency, elevated alkaline phosphatase levels, deranged renal function tests and arterial blood gas analysis suggestive of metabolic acidosis. Bilateral lower limb scanogram (Figure 3) showed classical signs of rickets such as splaying, fraying and cupping at the metaphysis along with bilateral genu valgum. Ultrasonography of both kidneys showed raised cortical echogenicity. Cortico-medullary differentiation was lost. There was no hydronephrosis or calculus. These changes were suggestive of grade III chronic renal parenchymal disease. Her sexual development was consistent with her pre-pubertal stage.
Table 1. Laboratory investigations of the patient.
| Laboratory Test |
Patient’s value |
Reference range |
| Ionic Calcium |
1.03 |
1.12 - 1.32 mmol/L |
| Serum Calcium |
8.3 |
8.4 - 10.2 mg/dL |
| Serum Phosphorus |
4.6 |
3.0 - 5.0 mg/dL |
| Vitamin D3 (25 hydroxy Vit D) |
8.34 |
severe deficiency < 10 ng/mL |
| Serum Alkaline Phosphatase |
2120 |
75 - 875 IU/L |
| Parathyroid Hormone |
481.80 |
10 - 65 pg/mL |
| Thyroid stimulating hormone |
4.72 |
0.6 - 4.84 µIU/mL |
| Free T4 |
1.15 |
0.9 - 1.67 ng/dL |
| Kidney Function Tests |
| Blood Urea |
79 |
10 - 50 mg/dL |
| Serum Creatinine |
2.31 |
0.5 - 1.2 mg/dL |
| Serum Uric Acid |
4.4 |
2.0 - 7.0 mg/dL |
| Serum Sodium |
141 |
135 - 145 mEq /L |
| Serum Potassium |
4.0 |
3.5 - 5.5 mEq /L |
| Serum Chloride |
113 |
98 - 110 mEq /L |
| Arterial Blood Gas Analysis |
| pH |
7.19 |
|
| pCO2 |
24 |
35 - 45 mm of Hg |
| pO2 |
75 |
80 - 100 mm of Hg |
| Bicarbonate |
9.2 |
22 - 26 mmol/L |
| Base Excess |
-19 |
between -3 and +3mmol/L |
| Lactate |
1.8 |
0.5 - 1.6 mmol/L |
| Random blood Glucose |
81 |
70 -110 mg/dL |
Figure 1. Congenital left sided complete cleft lip and complete cleft palate
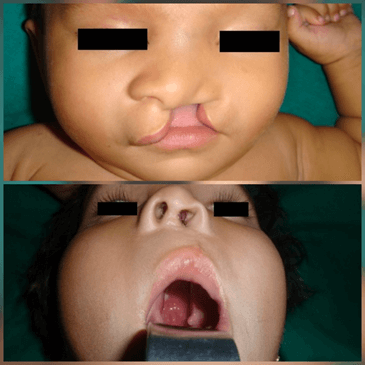
Figure 2. Post axial polydactyly of both upper limbs and both lower limbs

Figure 3. Marked truncal obesity and Bilateral lower limb scanogram showing bilateral genu valgum along with classical features of rickets.
|
| |
What is the diagnosis?
|
|
|
Discussion
Bardet-Biedl Syndrome (BBS). BBS is a rare ciliopathic autosomal recessive genetic disorder with multi-system impairment primarily characterized by obesity, retinal dystrophy, polydactyly, learning difficulties, hypogonadism and renal malformations.1 The diagnosis of BBS is based on the diagnostic criteria2 which depends predominantly on the clinical features. For the diagnosis of this syndrome, at least four major or three major and two minor features must be found in a patient. Our patient had five primary features such as retinitis pigmentosa, polydactyly, obesity, learning disabilities, renal dysfunction and five secondary features such as speech and developmental delay, astigmatism, brachydactyly, hypodontia and high arched palate (Table 2).
As per the published reports, less than 15 cases of BBS are reported from India1, out of which most of cases are picked up post-pubertally, which makes this case unique. Secondary features of BBS include speech delay, development delay, congenital heart disease, hepatic fibrosis, strabismus or cataract, neurological deficits, dental anomalies, diabetes mellitus and hypertension.1,2 Apart from the secondary features, our patient had a congenital left sided complete cleft lip and palate which is not reported in any literatures associated with BBS. So far, only 3 cases of BBS has been reported to have chronic kidney disease (CKD) from India, which initially goes undetected.3 Our case report was also similar in terms of deranged renal function tests and sonographically supported evidence of grade III chronic renal parenchymal disease with loss of cortico-medullary differentiation. Bilateral genu valgum in the child was attributed to the nutritional cause of Vitamin deficiency more than a renal cause which is chronic kidney disease (CKD) due to highly elevated alkaline phosphatase levels (>2000 IU/L). Vitamin D deficiency in this case was due to trapping of Vitamin D in the excess adipose tissue and the insufficient lipolytic stimulation causing immobilization of Vitamin D from the fat cells.4
Table 2. Diagnostic features of Bardet- Biedl Syndrome identified in our patient.1
| Primary features |
Our Case |
| Four features are required to be present of the following: |
|
| Rod-cone dystrophy |
+ |
| Polydactyly |
+ |
| Obesity |
+ |
| Learning disabilities |
+ |
| Hypogonadism in males or genital abnormalities in females |
|
| Renal dysfunction |
+ |
| Secondary features |
| Speech disorder/delay |
+ |
| Serum Creatinine |
+ |
| Astigmatism |
+ |
| Brachydactyly/syndactyly |
+ |
| Developmental delay |
+ |
| Polyuria/polydipsia (nephrogenic diabetes insipidus) |
|
| Ataxia/poor coordination/imbalance |
|
| Mild spasticity (especially lower limbs) |
|
| Diabetes mellitus |
|
| Hypodontia and high arched palate |
+ |
| Left ventricular hypertrophy/congenital heart disease |
|
| Hepatic fibrosis |
|
Note: For Diagnosis of Bardet Biedl syndrome, at least four major or three major and two minor features are required.
Among all the diagnostic features of BBS, the leading cause of morbidity and mortality is renal failure, where 25% die by the age of 44 years, hence such cases warrants attention.5 These cases require a multi-disciplinary approach of management. The index case was advised to wear glasses for myopic astigmatism, speech therapy and to lose weight through proper controlled diet and exercises. Parents of the child were counselled for regular follow up to observe for response to treatment for rickets and metabolic acidosis, to watch for progressive renal changes, worsening visual disturbances, to monitor the blood pressure values, to prevent future development of diabetes mellitus and other metabolic syndrome complications. Though this patient had multiple consultations by several specialists in different facilities, the diagnosis had been missed, probably because of the rarity of this condition and by owing to the slow emergence of features like learning disabilities, retinitis pigmentosa and renal dysfunction. This index case warrants every pediatrician to track such doubtful cases on a long term basis.
|
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
- Hooda AK, Karan SC, Bishnoi JS, Nandwani A, Sinha T. Renal transplant in a child with Bardet-Biedl syndrome: A rare cause of end-stage renal disease. Indian J Nephrol 2009;19 :112-114. [CrossRef] [PubMed] [PMC free article]
- Beales PL, Elcioglu N, Woolf AS, Parker D, Flinter FA. New criteria for improved diagnosis of Bardet-Biedl syndrome: results of a population survey. J Med Genet. 1999;36: 437-446.
- Kute VB, Vanikar AV, Gumber MR, Patel HV, Shah PR, Patil SB, et al. Bardet-biedl syndrome: a rare cause of chronic kidney disease. Indian J Clin Biochem. 2013;28:201-205. [CrossRef] [PubMed] [PMC free article]
- Migliaccio S, Di Nisio A, Mele C, Scappaticcio L, Savastano S, Colao A; Obesity Programs of nutrition, Education, Research and Assessment (OPERA) Group. Obesity and hypovitaminosis D: causality or casualty? Int J Obes Suppl. 2019;9:20-31. [CrossRef] [PubMed] [PMC free article]
- Forsythe E, Sparks K, Best S, Borrows S, Hoskins B, Sabir A et al. Risk factors for severe renal disease in Bardet-Biedl syndrome. J Am Soc Nephrol. 2017;28:963-970 [CrossRef] [PubMed] [PMC free article]
|
|
| |
Cite this article as:
Khamkar A M, Jose G E, Pote P D, Suryawanshi P. Knocking Down the Diagnosis in Knock Knees. Pediatr Oncall J. 2021;18: 102-104. doi: 10.7199/ped.oncall.2021.35
|