April Oertle1, Justin Assioun2,3, Stephanie Schroter2,3.
1University of Illinois College of Medicine, Rockford, Illinois, USA,
2Division of Emergency Medicine, Rady Children’s Hospital San Diego, San Diego, California, USA,
3Department of Pediatrics, University of California, San Diego School of Medicine, La Jolla, California, USA.
ADDRESS FOR CORRESPONDENCE
April Oertle, 6229 Parks Edge Dr, Loves Park, 61111, Unites States.
Email: Aoertl2@uic.edu | | Abstract | | Atrioventricular (AV) block, characterized by delayed or interrupted transmission of electrical impulses, rarely occurs in structurally normal hearts. Mobitz type II AV block, a specific form of second-degree heart block, is rarely seen in children and is often associated with underlying cardiac pathology. We present a case of a 14-year-old male with a structurally normal heart who exhibited paroxysmal variable second degree (Mobitz type II) arrhythmia. Initial concerns of hypertrophic cardiomyopathy were raised due to high lateral lead voltages on electrocardiogram and signs of heart block on telemetry. However, further evaluation revealed no structural abnormalities. Extensive diagnostic workup, including cardiac magnetic resonance imaging and laboratory testing ruled out ischemia, myocarditis, autoimmune pathology, Lyme, and Chagas disease. The patient demonstrated stable hemodynamics but required continuous monitoring due to potential progression to complete heart block. This case highlights the need to consider various differential diagnoses in pediatric patients with cardiac conduction abnormalities, especially without structural heart disease. | | | | Keywords | | Mobitz Type II, 2nd degree AV block, AV block, cardiac conduction disorders, sinus node dysfunction. | | | | Introduction | Cardiac conduction disorders manifesting in the pediatric population are uncommon, especially in children without a history of structural heart disease.1 Primary arrhythmias are rarely documented in children, though they may occur in a structurally normal heart or with an associated congenital heart disease.2 Atrioventricular (AV) block occurs when there is a delay or interruption in the transmission of electrical impulses from the upper chambers (atria) to the lower chambers (ventricles) of the heart.3 This condition can result from various factors, including structural cardiac abnormalities or dysfunction within the heart’s conduction system, leading to compromised heart rhythm regulation. Disturbances in cardiac conduction can manifest as either transient or permanent conditions, presenting clinically with varying degrees of delay, intermittency, or absence in the transmission of electrical impulses.3 First-degree AV block refers to delay in the conduction from the atrium to the ventricle, characterized by a prolonged PR interval exceeding 200 milliseconds, without complete interruption.3 Second-degree AV block involves intermittent transmission of atrial impulses to the ventricles and is further classified into Mobitz type I (Wenckebach Block or Phenomenon), Mobitz type II or two-to-one or higher AV block. Second degree AV blocks often display a pattern such as a 2:1 or 3:23. For example, in cases of 2:1 AV block, a ventricular complex (QRS, T) follows every second atrial (P) complex. In Mobitz type II AV block, the PR interval is consistent prior to the P wave that fails to conduct to the ventricles3 (Figure 1). Mobitz type II most commonly occurs below the AV node, in the bundle of His or even in the right and left bundle branches (Figure 1). In third degree AV block no atrial impulses are conducted to the ventricles of the heart.
Figure 1. Diagram of heart with normal anatomy4, from Cleveland Clinic.
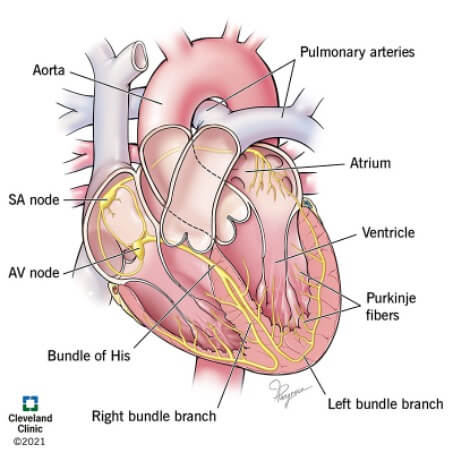
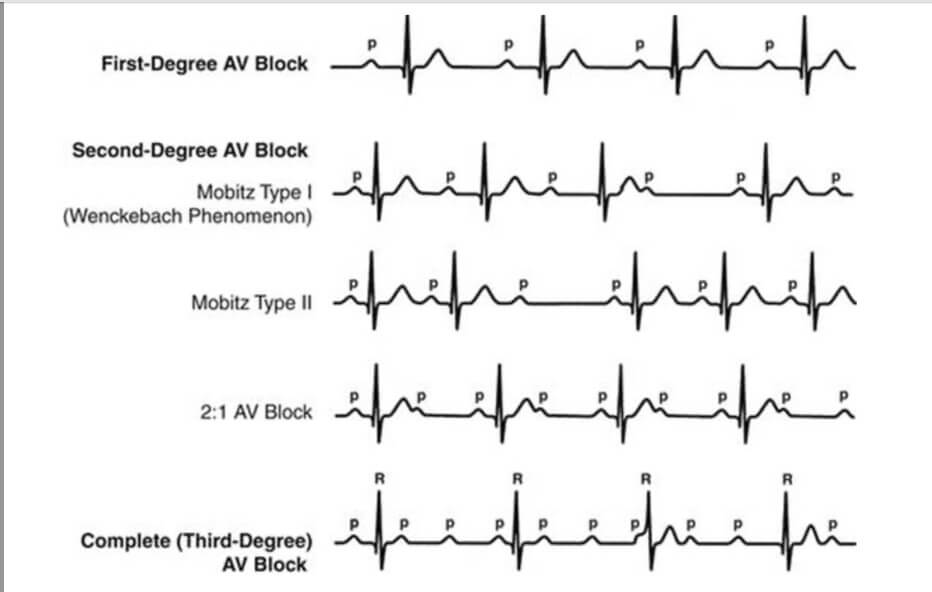
Figure 2. A single lead EKG showing the different types of AV block.5 In Mobitz type II second degree AV block, the first and fifth P waves are not conducted through the AV node.3 There is no QRS complex that follows the P wave. The PR interval is unchanged prior to the non-conducted beats. Image courtesy of: Park MK, Guntheroth WG: How to Read Pediatric ECGs, 4th ed. Philadelphia, Mosby, 2006.
Almost all Mobitz type II presentations are due to the presence of cardiac disease such as myocardial ischemia, fibrosis, myocarditis, Lyme disease, cardiomyopathy, cardiac tumors, collagen vascular disorders, or hyperthyroidism.6 It seldomly occurs in individuals lacking pre-existing heart pathology. Reversible factors often linked with this type of blockage include myocardial infarction causing ischemia in the AV node and medications that affect conduction within the AV node, such as digoxin, beta blockers, and calcium channel blockers.3 Mobitz type II has an increased risk of progression to complete AV block. Therefore, the treatment for Mobitz type II often requires pacemaker placement and lifelong follow up.6 We present a rare case of a child with a structurally normal heart, without comorbidities, who was found to have variable Mobitz type II AV block on presentation.
| | | | Case Report | A 14-year-old, fully vaccinated, male with no past medical history was transferred from an adult emergency department to a Level 1 pediatric emergency department (PED) with concerns for hypertrophic cardiomyopathy due to high lateral lead voltages on initial electrocardiogram (EKG) which progressed to signs of variable Mobitz type II heart block noted on telemetry.
His chief complaint was a “funny sensation” over his left chest when going to sleep. The sensation was not painful, did not feel like palpitations, or feel like his heart was skipping a beat. He denied any shearing pain radiating to his back. He denied associated diaphoresis, shortness of breath, abdominal pain, nausea, and vomiting. The parents endorse that the child is an athlete and has never experienced any dizziness, prior syncopal episodes or other exertional symptoms. The patient did not report symptoms of diminished exercise tolerance or fatigue. He denied blunt trauma to his chest.
On further review of systems, he denied any fevers, sore throat, recent illnesses, or history of tick bites or travel to wooded areas or camping. He denied any use of illicit substances and was not taking any daily medications. He was not taking any other vitamins, herbal supplements, or teas. He had not received any recent vaccines.
Family history was negative for congenital heart disease, early cardiac disease, or unexplained sudden deaths. His paternal grandfather had a pacemaker implantation in his 60s, for an unknown reason. There was no other family history of syncope, deafness, seizures or maternal history of rheumatic or other autoimmune diseases. Of potential significance, the family is from a big city in Brazil with a recent as well as frequent visits back to Brazil. However, they reside in the United States.
On arrival to the PED, he was hemodynamically stable. His heart rate was 90 beats per minute (BPM), blood pressure was 132/65 mmHg, respiratory rate of 18 breaths/minute, and his oxygen saturation was 99% on room air. Physical exam was overall unremarkable, with normal S1 and S2, no S3 or S4 sounds. There was a I/VI soft coarse systolic murmur heard only at right upper sternal border into the neck. There was no diastolic murmur. There was no reproduceable chest pain and no clubbing of fingers or toes. Lung sounds were clear to auscultation bilaterally with no evidence of respiratory distress. No hepatomegaly palpated on exam.
Initial EKG, at the adult emergency department, showed concern for high voltages in the lateral leads (Figure 3). Prior to transfer, the patient was noted to have a variable Mobitz type II patterned arrhythmia on continuous telemetry (Figures 4, 5). On arrival to the PED, an EKG was done and is shown below in Figure 6, which show sinus rhythm with occasional premature ventricular complexes.
Figure 3. Initial presentation from adult hospital, with concerns of left ventricular hypertrophy.
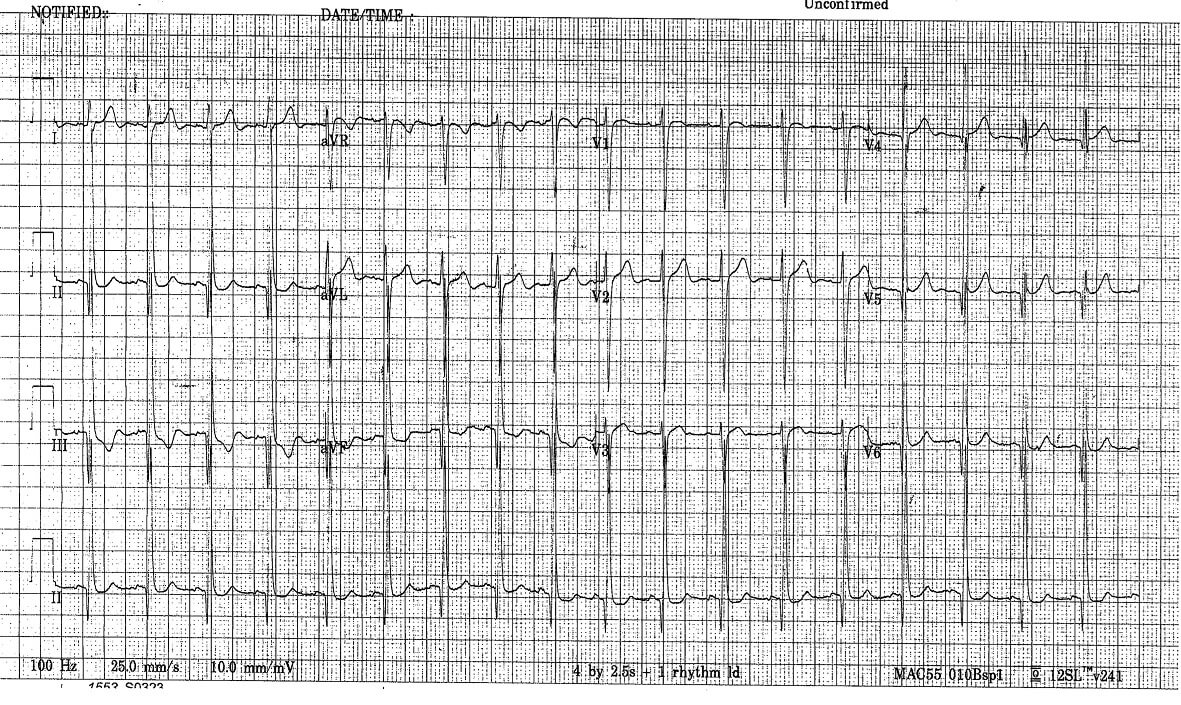
Figure 4. Rhythm strips that show variable Mobitz type II.
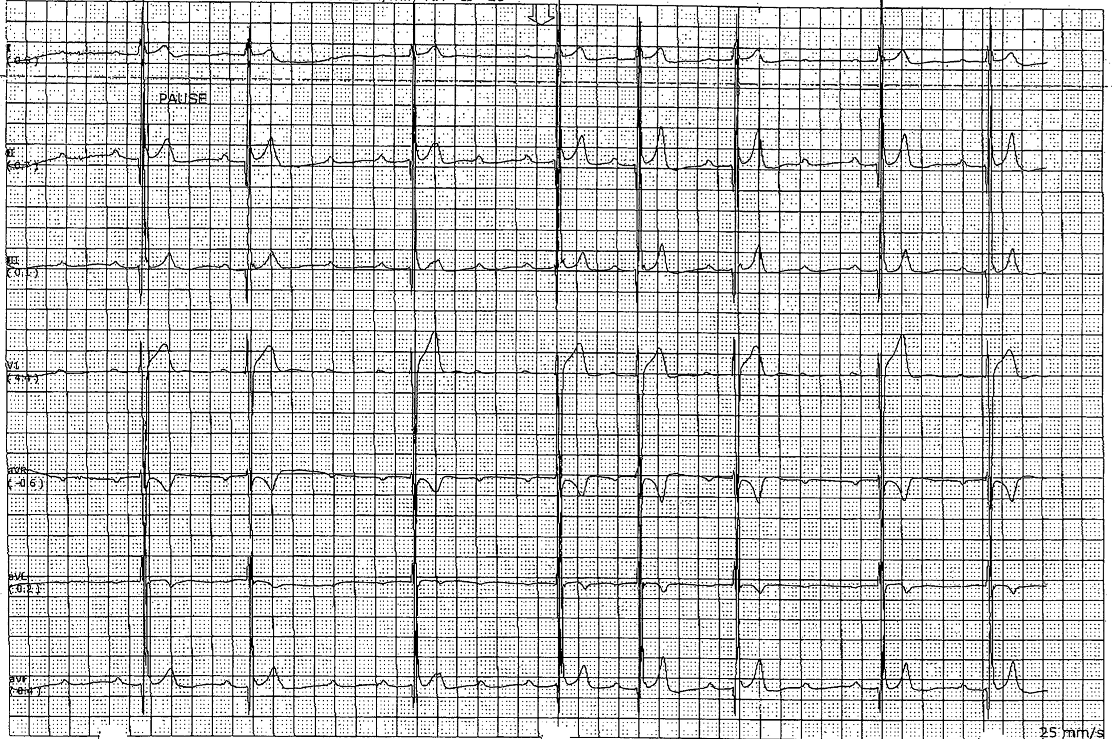
Figure 5. Rhythm strips that show variable Mobitz type II.
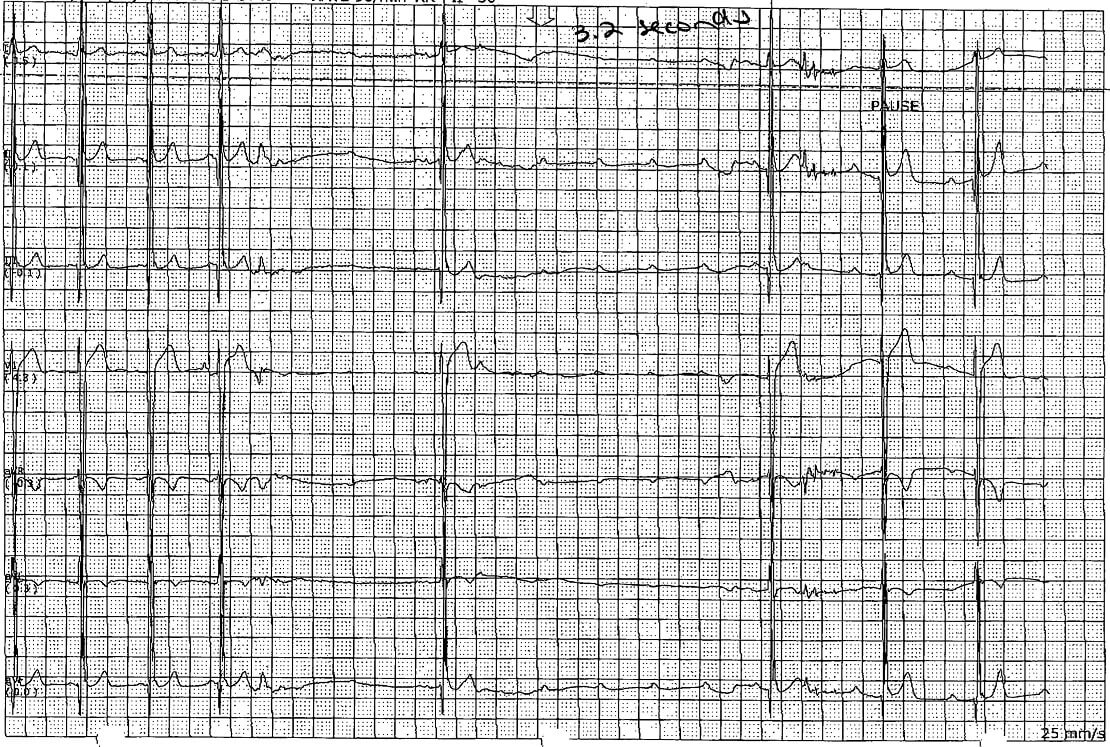
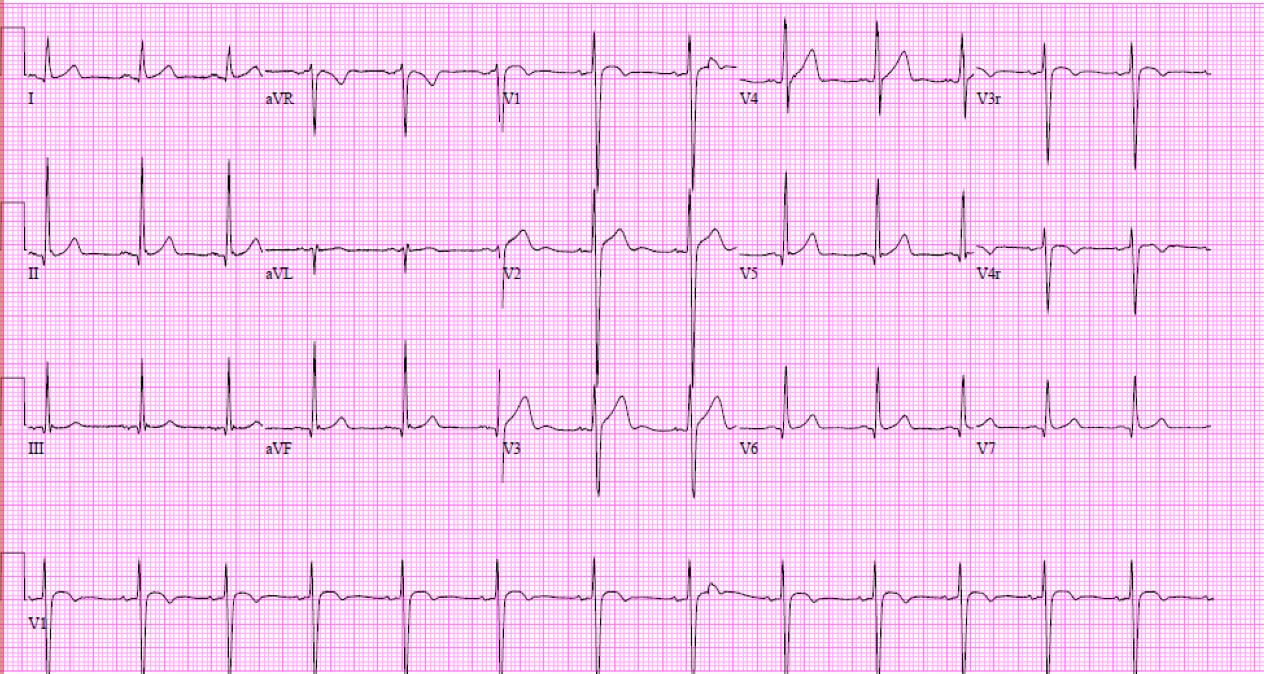
Figure 6. Normal sinus rhythm. Possible left ventricular hypertrophy. First EKG at PED.
Given the EKG findings, cardiology was consulted on arrival and the following labs were obtained: complete blood count with differential (CBCd), complete metabolic panel (CMP), erythrocyte sedimentation rate (ESR), c-reactive protein (CRP), troponin I, brain natriuretic peptide (BNP), which had no significant abnormalities. Specifically, the troponin I level, a crucial biomarker associated with cardiac damage, was measured at less than 0.01 ng/mL (normal <0.05 ng/mL), further confirming the absence of myocardial ischemia at that time. Additionally, the EKG results did not exhibit any discernible signs of acute or prior ischemic myocardial injury. BNP was 11 pg/mL (normal <100 pg/mL). Urine drug screen was negative. Laboratory tests that resulted after emergency department evaluation included negative: Sjogren’s antibodies (SS-A/SS-B), echovirus antibody panel, and Lyme antibody screen.
Chest X-Ray was normal with no signs of cardiomegaly or pulmonary congestion. The patient was admitted to the cardiology service for further evaluation. On admission, echocardiogram (ECHO) and cardiac MRI demonstrated a normal left ventricular size, normal left ventricular systolic function, and a left ventricular ejection fraction of 59%. Right ventricular size and right ventricular systolic function were also normal with an ejection fraction of 54%. There was no evidence of segmental or diffuse myocardial fibrosis on post-contrast late gadolinium enhancement imaging.
Exercise Stress test demonstrated a VO2 peak of 60.5 ml/kg/min (111% of predicted value for age). Patient maintained sinus rhythm with intact AV conduction throughout test with a peak heart rate of 197 bpm. Patient also exhibited normal pulmonary function test pre- and post-exercise.
The patient completed three-day event patch monitoring which demonstrated sinus rhythm most of the time with rare premature atrial contractions, rare premature ventricular contractions, rare Mobitz I (Wenckebach) block, and brief 2:1 AV Block overnight. An implantable loop recorder was placed (ILR) and has detected six sinus pauses >3 seconds, but no further Mobitz II AV block, or other abnormal tachyarrhythmias, bradyarrhythmias, or atrial fibrillation. Follow-up includes monthly ILR checks, with electrophysiology clinic every six months. One year post-presentation, the patient, an otherwise healthy athlete, remains asymptomatic. | | | | Discussion | Cardiac conduction disorders are uncommon in neonates and children.7 Congenital heart block occurs in approximately 1 per 15,000 to 20,000 live births.8 It is termed congenital when detected in utero, at birth, or within the initial month of life. Childhood AV block manifests sometime between one month of age and up to 18 years of life. This condition may arise independently in a structurally normal heart.7,8 Symptomatic patients require cardiac pacing, while asymptomatic individuals may benefit from prophylactic pacing to mitigate the risk of sudden death.7 Advanced second or third-degree AV block is one of the most common indications for permanent pacemaker implantation in children.9
For a pediatric patient presenting with heart block, a comprehensive set of laboratory tests is essential to elucidate the underlying etiology, guide management, and determine prognosis. Initial evaluation should include a CBC and CMP to assess for systemic involvement and metabolic disturbances that could contribute to or result from the heart block. Electrolyte imbalances, particularly abnormalities in potassium, calcium, and magnesium, can significantly affect cardiac conduction and must be identified and corrected.10 Additionally, assessment of renal and hepatic function through the CMP can reveal potential secondary cases of heart block such as uremia or hepatic dysfunction.11
To investigate infectious and inflammatory causes, testing for markers of inflammation (e.g. CRP, ESR) and specific infections is important. Serological tests for Lyme disease should be considered, especially in endemic areas, given its association with heart block. Furthermore, autoantibody testing, including anti-Ro/SSA and anti-La/SSB antibodies, is warranted to evaluate for underlying autoimmune conditions.7 Thyroid function tests (TSH, free T4) should be performed to exclude thyroid dysfunction, as both hyperthyroidism and hypothyroidism can impact cardiac conduction and cause heart block.12 Thyroid function tests were normal in our case.
Additionally, genetic testing may be indicated, particularly in cases of congenital heart block or when there is a family history suggestive of inherited arrhythmias.2 Our patient did not have a family history suggesting a cardiac disorder. Lastly, in cases of suspected cardiomyopathy, cardiac biomarkers such as BNP or N-terminal pro-BNP (NT-proBNP) can provide information on the degree of cardiac involvement and heart failure.13 Collectively, these laboratory investigations provide a comprehensive approach to diagnosing the etiology of heart block in pediatric patients, allowing for targeted therapeutic interventions and better-informed prognostic assessments.
Mobitz type II AV block, a specific form of second-degree heart block, is relatively rare in the pediatric population. Whereas Mobitz type I block can be a normal finding during sleep.14 Mobitz type II is generally accepted to be pathologic and has the potential to progress to complete heart block.6 We were unable to find any studies on the prevalence or incidence of Mobitz type II AV blocks in the pediatric population and more specifically in pediatric patients with a structurally normal heart.
Patients diagnosed with Mobitz type II second degree AV block commonly exhibit a range of symptoms. The absence of one or more P waves conducting to the ventricles can precipitate fatigue, dizziness, presyncope, or syncope, commonly known as Stokes-Adams attacks.2 This phenomenon arises from the inherently slower intrinsic cardiac pacemakers in the ventricles compared to those in the atria. Furthermore, apart from the irregular pulse and potential bradycardia, physical exam findings are often nonspecific.3 Notably, individuals with infrequently nonconducted P waves and a normal sinus heart rate may experience minimal or no symptoms.3 However, if the baseline heart rate is already displaying sinus bradycardia, this can lead to a significant decrease in cardiac output.3 The decrease in cardiac output can result in cardinal signs of inadequate blood flow or heart failure. Interestingly, in our case the patient only complained of a new onset ill-defined “funny sensation” while falling asleep.
Exercise stress testing is valuable for identifying the location and severity of AV blockages.6 Typically, supra-His blockages improve during exercise due to heightened sympathetic activity.6 If second or third-degree AV blockages occur during exercise, it suggests a disruption in the His-Purkinje system’s conduction.6 Elevations in heart rate, such as induced by physical exertion, administration of atropine, or atrial pacing have the potential to exacerbate Mobitz type II second-degree AV block.3 In this condition, the increased heart rate can accentuate the blockage of electrical impulses between the atrial and ventricles, intensifying the disruption in cardiac conduction and potentially leading to more pronounced symptoms.3
Familial AV conduction block is associated with a genetic predisposition. This condition has been found to be linked with various mutations in the SCN5A gene.2 These genetic alterations contribute to disruptions in AV conduction, highlighting the complex interplay between inherited traits and cardiac function. No cardiac genetic testing has been done on our patient to date. Autoimmune-mediated congenital AV block is linked with a substantial neonatal mortality rate, with 5% to 30% of cases progressing to dilated cardiomyopathy, highlighting the critical need for early detection and prevention.7 Sporadically, pediatric patients may present with AV block of unknown etiology, devoid of maternal antibodies, structural cardiac anomalies, or discernible causes. The scientific literature concerning the origin and clinical progression of these cases of apparent idiopathic heart block is notably limited. However, a pioneering study conducted by Barteau et al., investigating the heritability of pediatric idiopathic heart block, revealed compelling evidence of a significant genetic predisposition underlying congenital and childhood nonimmune isolated AV block.15 This underscores the importance for physicians at all levels to consider familial screening, as it may yield substantial insights into heritability, even in instances where the condition initially manifests as sporadic and appears idiopathic.3
The majority of Mobitz type II presentations can be attributed to the existence of cardiac diseases, including but not limited to myocardial ischemia, fibrosis, myocarditis from Lyme disease, various forms of cardiomyopathy, cardiac tumors, collagen vascular disorders, and hyperthyroidism.15 HCM is a rare but significant cardiac condition in children, characterized by asymmetric hypertrophy of the left ventricle.16 While HCM primarily affects the structure of the myocardium, its consequences often extend to the electrical conduction system of the heart. This can potentially lead to heart block, bradycardia, or sudden cardiac death.16 For our patient, the ECHO and cardiac MRI results revealed a normal cardiac profile, characterized by the absence of any indications of left ventricular hypertrophy or HCM. This diagnostic assessment provided reassurance regarding the structural integrity and function of the child’s heart, indicating that there are no apparent abnormalities in the size or thickness of the left ventricle. There was no evidence of cardiac tumors or myocardial fibrosis, eliminating concerns related to neoplastic growths that could impact the heart’s structure and function.
AV conduction disorders have been observed in conjunction with acquired cardiac pathologies, exemplified by conditions such as Lyme disease, Kawasaki disease (KD), and Chagas disease.3
Lyme disease, caused by the Borrelai burgdorferi bacterium, can lead to Lyme carditis which manifests days to months after initial exposure to the bacterial spirochete.17 The patient’s Lyme antibody titers were negative. With a lack of detectable Lyme antibodies and the absence of historical risk factors, the possibility of Lyme disease as an underlying cause for the cardiac conduction abnormality was effectively eliminated.
Similarly, KD, the most recognized vasculitis of childhood is characterized by systemic inflammation of small and medium sized vessels which may incite inflammation in the coronary arteries; it is a leading cause of acquired pediatric heart disease.18 Kawasaki disease (KD) typically presents with high fever, mucocutaneous inflammation, and cervical lymphadenopathy, primarily affects the coronary arteries and other cardiovascular structures. KD was eliminated from the differential due to the lack of high fevers in the patient’s history, negative findings on physical exam (no characteristic signs: extremity changes, rash, erythema of lips and oral mucosa, conjunctival irritation, lymphadenopathy) and he did not meet KD criteria on laboratory evaluation (normal white blood cell count, CRP< ESR).19
Additionally, a neglected tropical disease, Chagas disease, caused by the protozoan Trypanosoma cruzi, is notorious for its chronic cardiomyopathic effects, which can impair the conduction of electrical signals within the heart.20 Cardiac symptoms of chronic Chagas disease can include arrhythmias, heart failure, and sudden death. Our patient had a recent trip to Brazil and frequently visits family in Brazil where Chagas disease is endemic.21 Therefore, Chagas disease was added to the differential. The patient did not have a history of fevers, headaches, fatigue, nausea, or vomiting. The patient’s physical exam was negative for hepatosplenomegaly, skin rashes, or swollen lymph nodes. Additionally, there were no signs or symptoms of myocarditis, megaesophagus, or megacolon. Furthermore, the patient only travelled to major cities in Brazil. Therefore, Chagas disease was lower on the differentials as etiology to the patient’s arrythmia and has not been tested to date.
Unstable patients with Mobitz type II second-degree AV block require urgent treatment, typically involving beta-adrenergic agonists like isoproterenol, dopamine, dobutamine, or epinephrine, along with temporary cardiac pacing. Hemodynamically unstable signs include hypotension, altered mental status, shock, and ongoing chest pain.3 Stable patients do not require immediate therapy but should be continuously monitored with transcutaneous pacing pads in place due to the instability of Mobitz type II block, which often progresses to complete AV block.3 Complications can include sudden cardiac death. Our patient had an ILR placed and has been hemodynamically stable. Monthly ILR evaluations have revealed 6 sinus pauses following the loop recorder implantation, with no other arrhythmias noted.
In most cases, individuals with non-reversible AV node disease require the implantation of a permanent pacemaker.3 However, the patient did not receive a pacemaker as they did not meet Class I indications for emergent pacemaker intervention, primarily due to the infrequent nature of their sinus node dysfunction (SND).9 SND refers to physiologically inappropriate atrial rates, either due to abrupt pauses or sustained bradycardia.9 Class 1 SND is when there is a correlation between the symptoms with age-inappropriate bradycardia.9 Current guidelines emphasize that sinus pauses alone are no longer absolute indications for pacemaker placement.9 In this case, a pacemaker would only be considered reasonable (Class IIa) if no reversible or secondary etiologies were identified and the patient experienced symptoms during exercise, or possibly (Class IIb) if they had minimal unexplained symptoms.9
A comprehensive second-pass workup, including normal cardiac magnetic resonance imaging and an exercise stress test that demonstrated a maximal heart rate of 197 beats per minute without cardiac symptoms, further supported the decision against immediate pacemaker intervention. Given these findings, the pediatric electrophysiology team discussed an ILR to monitor for recurrence of AV block and other potential symptoms, which the family opted for instead of a leadless pacemaker. Six-month follow-ups with the pediatric electrophysiology clinic continue to report stable findings and no new abnormalities. | | | | Conclusion | | The presented case of a 14-year-old male with a structurally normal heart who was diagnosed with a high-grade variable (1:1 or 5:1) Mobitz type II arrhythmia highlights the complexity and diversity of conduction disorders in the pediatric population. Mobitz type II heart block is an uncommon condition, especially in children. The case emphasizes the importance of considering a broad differential diagnosis. While many etiologies and differentials have been ruled out in this patient, the etiology to his arrythmia remains unknown. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Brucato, A., A. Jonzon, Friedman, D., Allan, L. D., Vignati, G., Gasparini, M., Stein, J. I., Montella, S., M. Michaelsson, & J. Buyon. (2003). Proposal for a new definition of congenital complete atrioventricular block. Lupus, 12(6), 427-435. https://doi.org/10.1191/0961203303lu408oa. [CrossRef] [PubMed]
- Mangi, M. A., Jones, W. M., Mansour, M. K., & Napier, L. (2023). Second-Degree Atrioventricular Block. PubMed; StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK482359/
- Baruteau, A.-E., Pass, R. H., Thambo, J.-B., Behaghel, A., Le Pennec, S., Perdreau, E., Combes, N., Liberman, L., & McLeod, C. J. (2016). Congenital and childhood atrioventricular blocks: pathophysiology and contemporary management. European Journal of Pediatrics, 175(9), 1235-1248. https://doi.org/10.1007/s00431-016-2748-0. [CrossRef] [PubMed] [PMC free article]
- Cleveland Clinic. (2021). Heart Conduction: What Is It & How It Works. Cleveland Clinic. https://my.clevelandclinic.org/health/body/21648-heart-conduction-system.
- Park, M. K., & Guntheroth, W. G. (2006). How to read pediatric ECGs. Mosby/Elsevier.
- Saleh, F., Greene, E. A., & Mathison, D. (2014). Evaluation and management of atrioventricular block in children. Current Opinion in Pediatrics, 26(3), 279-285. https://doi.org/10.1097/mop.0000000000000100. [CrossRef] [PubMed]
- Brucato, A., et al. "Proposal for a New Definition of Congenital Complete Atrioventricular Block." Lupus, vol. 12, no. 6, June 2003, pp. 427-35. DOI.org (Crossref), https://doi.org/10.1191/0961203303lu408oa. [CrossRef] [PubMed]
- Bordachar, P., Zachary, W., Ploux, S., Labrousse, L., Haissaguerre, M., & Thambo, J.-B. (2013). Pathophysiology, clinical course, and management of congenital complete atrioventricular block. Heart Rhythm, 10(5), 760-766. https://doi.org/10.1016/j.hrthm.2012.12.030. [CrossRef] [PubMed]
- Shah, M. J., Silka, M. J., Silva, J. R., Balaji, S., Beach, C., Benjamin, M., Berul, C. I., Cannon, B. C., Cecchin, F., Cohen, M. J., Dalal, A., Dechert, B. E., Foster, A., Gebauer, R., Gonzalez, C., Kannankeril, P. J., Karpawich, P. P., Kim, J., Mani Ram Krishna, & Kubuš, P. (2021). 2021 PACES Expert Consensus Statement on the Indications and Management of Cardiovascular Implantable Electronic Devices in Pediatric Patients. JACC: Clinical Electrophysiology, 7(11), 1437-1472. https://doi.org/10.1016/j.jacep.2021.07.009. [CrossRef] [PubMed]
- Fisch, C. (1973). Relation of Electrolyte Disturbances to Cardiac Arrhythmias. Circulation, 47(2), 408-419. https://doi.org/10.1161/01.cir.47.2.408. [CrossRef] [PubMed]
- Mohler, H. K. (1929). Heart Block and Uremia. Journal of the American Medical Association, 92(9), 706. https://doi.org/10.1001/jama.1929.02700350014007. [CrossRef]
- Ata, F. (2024). Atrioventricular block in patients with hyperthyroidism: a narrative review. Journal of International Medical Research, 52(1). https://doi.org/10.1177/03000605231223040. [CrossRef] [PubMed] [PMC free article]
- Tsai, S.-H., Lin, Y.-Y., Chu, S.-J., Hsu, C.-W., & Cheng, S.-M. (2010). Interpretation and Use of Natriuretic Peptides in Non-Congestive Heart Failure Settings. Yonsei Medical Journal, 51(2), 151. https://doi.org/10.3349/ymj.2010.51.2.151. [CrossRef] [PubMed] [PMC free article]
- Adlakha, A., & Shepard, J. W. (1998). Cardiac arrhythmias during normal sleep and in obstructive sleep apnea syndrome. Sleep Medicine Reviews, 2(1), 45-60. https://doi.org/10.1016/s1087-0792(98)90053-3. [CrossRef] [PubMed]
- Alban-Elouen Baruteau, Albin Behaghel, Swanny Fouchard, Philippe Mabo, Schott, J.-J., Dina, C., Chatel, S., Villain, E., Jean-Benoit Thambo, François Marçon, Véronique Gournay, Rouault, F., Alain Chantepie, Guillaumont, S., François Godart, Martins, R. P., Béatrice Delasalle, Bonnet, C., Alain Fraisse, & Schleich, J.-M. (2012). Parental Electrocardiographic Screening Identifies a High Degree of Inheritance for Congenital and Childhood Nonimmune Isolated Atrioventricular Block. Circulation, 126(12), 1469-1477. https://doi.org/10.1161/circulationaha.111.069161. [CrossRef] [PubMed]
- Seggewiss, H., & Rigopoulos, A. (2003). Management of Hypertrophic Cardiomyopathy in Children. Pediatric Drugs, 5(10), 663-672. https://doi.org/10.2165/00148581-200305100-00002. [CrossRef] [PubMed]
- Bolourchi, M., Silver, E. S., & Liberman, L. (2018). Advanced Heart Block in Children with Lyme Disease. Pediatric Cardiology, 40(3), 513-517. https://doi.org/10.1007/s00246-018-2003-8. [CrossRef] [PubMed]
- Cohen, E., & Sundel, R. (2016). Kawasaki Disease at 50 Years. JAMA Pediatrics, 170(11), 1093. https://doi.org/10.1001/jamapediatrics.2016.1446. [CrossRef] [PubMed]
- Newburger, J. W., Takahashi, M., & Burns, J. C. (2016). Kawasaki Disease. Journal of the American College of Cardiology, 67(14), 1738-1749. https://doi.org/10.1016/j.jacc.2015.12.073. [CrossRef] [PubMed]
- Sabaini, B., Deorlan Pereira Dias, Márcia Moraes Cangussú, Porto, V., Daniel Dias Sampaio, & Luciano, F. (2023). Seroepidemiology of Chagas disease in at-risk individuals in Caraíbas, a city with high endemicity in Bahia State, Brazil. Frontiers in Public Health, 11. https://doi.org/10.3389/fpubh.2023.1196403. [CrossRef] [PubMed] [PMC free article]
- Forsyth, C. J., Manne-Goehler, J., Bern, C., Whitman, J., Hochberg, N. S., Edwards, M., Marcus, R., Beatty, N. L., Castro, Y., Coyle, C., Stigler-Granados, P., Hamer, D., Maguire, J. H., Gilman, R., & Meymandi, S. (2021). Recommendations for Screening and Diagnosis of Chagas Disease in the United States. The Journal of Infectious Diseases, 225(9). https://doi.org/10.1093/infdis/jiab513. [CrossRef] [PubMed] [PMC free article]
DOI: https://doi.org/10.7199/ped.oncall.2026.46
|
| Cite this article as: | | Oertle A, Assioun J, Schroter S. Mobitz Type II Cardiac Conduction Disorder in Adolescent Male. Pediatr Oncall J. 2024 Sep 24. doi: 10.7199/ped.oncall.2026.46 |
|