Ana Machado da Cunha1,2, Inês Mazeda2, Diogo Cunha Cabral3, Carolina Gonçalves2.
1Pediatric Department, Unidade Local de Saúde de Braga, Braga, Portugal,
2Pediatric Department, Unidade Local de Saúde de Póvoa de Varzim - Vila do Conde, Póvoa de Varzim, Portugal,
3ENT Department, Unidade Local de Saúde de Matosinhos, Matosinhos, Portugal.
ADDRESS FOR CORRESPONDENCE
Ana Isabel Machado da Cunha, Pediatric department, Unidade Local de Saúde de Braga, Sete Fontes – São Victor, 4710-243 Braga, Portugal.
Email: anamcunhaped@gmail.com | | Keywords | | Tornwaldt’s cyst, Nasopharynx, Syncope, MRI. | | | Tornwaldt's Cyst (TC), located on the posterior wall of the nasopharynx, is rarely diagnosed in the pediatric age group. It can be congenital or secondary to recurrent nasopharyngeal infections or trauma, such as chemoradiation or adenoidectomy.1,2 It is generally benign and typically asymptomatic, often discovered incidentally on imaging studies, so it does not require any therapeutic intervention. However, if it becomes symptomatic, surgical treatment is necessary, either through excision or marsupialization, leading to the complete resolution of symptoms in most patients.1,3
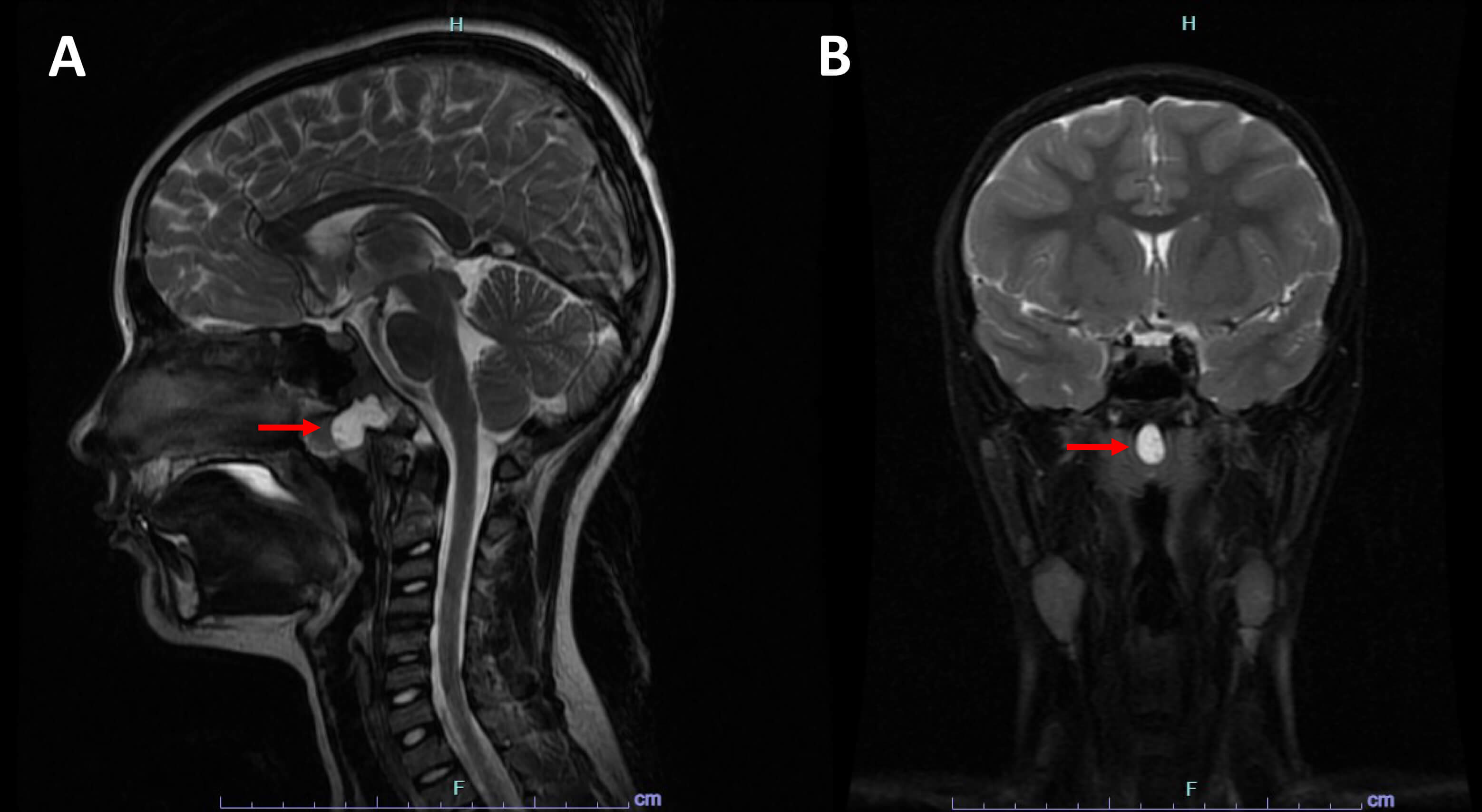
We describe the case of a 9-year-old male child, previously healthy, presented to Emergency Department due to two episodes of syncope on the same day. The first episode occurred after micturition and the second after defecation, both lasting less than 1 minute. Additionally, the patient reported rhinorrhea and nasal obstruction for the past 5 days and holocranial headache for the past day. No fever was reported. Prior to this episode, he had acute otitis media treated with amoxicillin and clavulanic acid, which ended 10 days prior. Upon admission, the patient was afebrile, had intact memory of the events and showed no abnormalities on physical or neurological examination. The electrocardiogram was normal. Blood tests revealed leukocytosis with neutrophilia and a slight increase in C-reactive protein. Other laboratory tests, including myoglobin, total creatine kinase, troponin and D-dimers, were normal. Abdominal ultrasound, echocardiogram and chest X-ray were unremarkable. A CT scan of the head was performed, showing no evidence of acute vascular lesion but revealing a hypodense oval formation in the roof of the nasopharynx, suggestive of a TC. The patient was examined by an otorhinolaryngologist (ENT), that described on nasal endoscopy marked adenoid hypertrophy with associated purulent exudate. The possibilities of an infected TC or adenoiditis was considered and intravenous (IV) antibiotic therapy with ceftriaxone was initiated. During the stay in the Emergency Department, the patient developed upper eyelid edema and erythema in the right eye, leading to the suspicion of right preseptal cellulitis. IV flucloxacillin was added for 3 days. On the 5th day of hospitalization, a contrast-enhanced MRI was performed, confirming the presence of a TC. (Figure 1) The patient completed 8 days of IV antibiotic and 8 days of oral antibiotic therapy. After discharge, the patient was referred to an outpatient ENT clinic for definitive surgical intervention.
Figure 1. Magnetic resonance imaging with contrast confirmed the presence of a Tornwaldt's cyst (red arrow). (A) Sagittal view. (B) Coronal view.
This case illustrates a clinical case of TC that manifested with syncope, an atypical presentation. There are reports of syncope associated with ENT procedures that involve nasopharyngeal stimulation, although the exact pathogenesis of neurally mediated syncope involving the nasopharynx is not clear.4,5 One possible mechanism associates the trigeminocardiac reflex with syncope. The classical mechanism of trigeminocardiac reflex suggests that mechanical stimulation of the trigeminal nerve or its peripheral branches leads to activation of the parasympathetic cardioinhibitory neurons of the vagus nerve. This stimulation can lead to bradycardia and, consequently, syncope.5 Although there is no literature data to corroborate the relationship between syncope and TC, in this case, we can correlate the underlying mechanism of syncope in the presented clinical with the presence of TC.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Alshuhayb Z, Alkhamis H, Aldossary M, Almoumen Z, Aldhurais A, Alshuhayb B, et al. .Tornwaldt nasopharyngeal cyst: Case series and literature review. Int J Surg Case Rep. 2020;76:166-169. DOI: 10.1016/j.ijscr.2020.09.105. [CrossRef] [PubMed] [PMC free article]
- Sekiya K, Watanabe M, Nadgir RN, Buch K, Flower EN, Kaneda T, et al. Nasopharyngeal cystic lesions: Tornwaldt and mucous retention cysts of the nasopharynx: findings on MR imaging. J Comput Assist Tomogr. 2014;38(1):9-13. DOI: 10.1097/RCT.0b013e3182a77699. [CrossRef] [PubMed]
- Marom T, Russo E, Ben Salem D, Roth Y. Nasopharyngeal cysts. International Journal of Pediatric Otorhinolaryngology. 2009; 73(8):1063-1070. DOI: 10.1016/j.ijporl.2009.01.004. [CrossRef] [PubMed]
- Wong A, Abu Bakar MZ. The nasocardiac reflex during nasoendoscopy: A commonly overlooked risk. Am J Otolaryngol. 2021;42(2):102869. DOI: 10.1016/j.amjoto.2020.102869. [CrossRef] [PubMed]
- Wang W, Cai H, Ding H, Xu X. Case report: 2 cases of cardiac arrest caused by rhino-cardiac reflex while disinfecting nasal cavity before endonasal transsphenoidal endoscopic pituitary surgery. BMC Anesthesiol. 2021;21(1):18. DOI:10.1186/s12871-021-01240-w. [CrossRef] [PubMed] [PMC free article]
DOI: https://doi.org/10.7199/ped.oncall.2026.8
|
| Cite this article as: | | Cunha A M d, Mazeda I, Cabral D C, Gonçalves C. Tornwaldt's Cyst - An unusual diagnosis with an atypical form of presentation. Pediatr Oncall J. 2026;23: 42-43. doi: 10.7199/ped.oncall.2026.8 |
|