Amit Chitalia, Ranjeet Togalkar, Kulbhushan Dagar.
Department of Pediatric Cardiac Services, Lotus children's hospital, Hyderabad, India.
ADDRESS FOR CORRESPONDENCE
Dr Amit Chitalia, Consultant Pediatric Cardiac Intensivist, Lotus children's hospital, #6-2-29, Lakdi ka pul, Hyderabad, Andhra Pradesh, India-500004
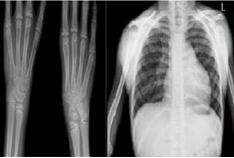
Email: dr.amit001@hotmail.com | | Keywords | | Holt Oram Syndrome, Heart-hand syndrome, Secundum atrial septal defect, Upper limb anomaly | | | A 12 year male child, presented with history of breathlessness (NYHA Grade: II/IV) and recurrent respiratory tract infections. Physical examination (Fig 1) revealed bilateral absent thumbs, short arms, unequal upper limb length (difference: 2.5 cm, left limb shorter), chest deformity, limited range of movement {in pronation of both upper limb}, drooping of shoulders and wide scapulae with normal lower limbs structurally and functionally, normal motor function, normal development and school performance, without any family history of such congenital anomaly. Radiological assessment showed bilateral absence of thumbs, fusion of carpal bones -capitate, trapezium, trapezoid in proximal row bilaterally, and scaphoid, lunate, triquetral in distal row of left hand with hypoplastic scapula, shallow glenoid, hypoplastic heads with overtubation of humeri .(Fig 2) Cardiovascular examination showed precordial bulge, wide and fixed split S2 with ejection systolic murmur of Grade III/VI in pulmonary area. Electrocardiogram showed prolonged P-R interval, frequent ventricular escape beats, varying degree of heart block, right axis deviation. Echocardiographic evaluation revealed moderate high ostium secundum atrial septal defect (ASD) with left to right shunt with mild pulmonary arterial hypertension. A 24 hour Holter study was performed which confirmed a bifascicular block, occasional premature ventricular and supraventricular beats, low grade ventricular arrhythmia and episodes of sinus bradycardia with junctional escape beats, all found as rarities with an isolated ASD. On detailed discussion with the electrophysiology teams across different institutions a conclusion was reached that these were primarily due to ventricular enlargement, so pacemaker implantation should be kept as a backup in view of the technical difficulties associated with the skeletal defects. The Secundum ASD was closed uneventfully with pericardial patch with four additional epicardial ventricular pacing wires in anticipation of conduction block in the post operative period. He had one episode of junctional ectopic tachycardia postoperatively, which was treated with core cooling, electrolyte correction and anti pyrexia measures. His hemodynamics improved henceforth and there were no further arrhythmias .The child needed aggressive lung physiotherapy during and after positive pressure ventilation in view of limited respiratory reserve. Child was discharged home at 5th post operative day in normal sinus rhythm with mild P-R prolongation. Before discharge detailed genetic counseling was done under which parents were informed regarding complete penetrance of the disease in autosomal dominant manner and need of complete evaluation of affected family members and progeny of the index case in future, possibly with fetal assessment. Pediatric orthopedic consultation was sought under which he was advised corrective limb surgery. The child is awaiting orthopedic correction and is undergoing extensive physiotherapy for prevention of contracture. At 6 month follow up, child is doing very well. Follow up ECG continues to exhibit regular sinus rhythm with resolution of P-R interval prolongation.
Figure 1: Skeletal features with surgical scar over sternum; post open heart surgery.

Figure 2: Typical radiological features of Holt Oram Syndrome
Holt-Oram Syndrome, also known as heart-hand syndrome is a rare autosomal dominant disorder characterized by distinctive upper limb skeletal anomalies, which are frequently associated with congenital heart disease and varying degrees of arrhythmias, was first reported in 1960 by Mary Clayton Holt and Samuel Oram. (1) Incidence of this condition is 1 per 100,000 births, equally affecting both sexes with over 300 cases reported in the literature worldwide (2,3) out of which surgically managed are very few. Molecular genetic studies have determined that mutations in the TBX3 and TBX5 (T-box 3-5) gene on chromosome 12q2, responsible for both the cardiac and skeletal manifestations in this rare genetic disorder. (4)
The typical combination is considered to be a triad, consisting of triphalangeal thumb, an Ostium Secundum ASD, with dysrhythmia of bizarre type as mentioned by Holt and Oram in 1960 (1,2) , and was typically found in the case presented here. But there happens to be a wide variation in extent of severity of both cardiac as well skeletal anomalies. Though almost always present, limb involvement varies from extremely subtle radiological findings like carpal bone fusion (sometimes only evident feature, one can find accidently in a radiograph) to severe limb anomalies like phocomelia & hypoplasia of various bones of upper limb. Radial bone anomaly is the commonest and left upper limb is more affected (3) than right, like found classically in presented case. Severity of cardiac malformation is not always proportional to upper limb deformity (5) and again varies from cardiac involvement ranged from asymptomatic conduction disturbances to multiple structural defects requiring surgery in infancy .(4) Sudden death could be caused by heart block. Defects ranges from an ASD of secundum type (being commonest 60%), Ventricular Septal Defect (VSD) (second common 18%) to more complex congenital heart lesions like Tetralogy of Fallot (TOF), and arch vena cava as well as great vessel anomaly of any severity and sometimes peripheral vessel abnormality. (5) Conduction disturbances may be due to genetic mutation itself and/or due to structural anomalies. As shown by the above case the need for a permanent pacemaker should be individualized as they can resolve after correction of the underlying cardiac defect. Prognosis is excellent, provided intervention is timely and multidisciplinary. (5)
Acknowledgements: We thank Dr. Roja T and Dr. Nadeem for radiological assessment, Dr. Anuradha for genetic counseling.
Contribution: AC conceived and designed the study and revised the manuscript for important content. He will act as guarantor of study. AC and KD were involved in management of the child. KD performed open heart surgery and helped in manuscript writing. RT conducted tests, collected data and helped in drafting paper. Final manuscript was approved by all.
Source of funding: nil
Competing of interest: nil
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Holt M, Oram S. Familial heart disease with skeletal malformations. Br Heart J. 1960; 22: 236-242. [CrossRef] [PubMed]
- Hurst JA, Hall CM, Baraitser M. The Holt-Oram syndrome. J Med Genet. 1991; 28: 406-410. [CrossRef] [PubMed]
- Newbury-Ecob RA, Leanage R, Raeburn JA, Young ID. Holt-Oram syndrome: a clinical genetic study. J Med Genet. 1996; 33: 300-307. [CrossRef] [PubMed]
- Bossert T, Walther T, Gummert J, Hubald R, Kostelka M, Mohr FW. Cardiac malformations associated with the Holt-Oram syndrome--report on a family and review of the literature. Thorac Cardiovasc Surg. 2002; 50: 312-314. [CrossRef] [PubMed]
- Basson CT, Cowley GS, Solomon SD, Weissman B, Poznanski AK, Traill TA, et al. The clinical and genetic spectrum of the Holt-Oram syndrome (heart-hand syndrome). N Engl J Med. 1994; 330: 885-891. [CrossRef] [PubMed]
|
| Cite this article as: | | Chitalia A, Togalkar R, Dagar K. Holt Oram Syndrome. Pediatr Oncall J. 2010;7: 112-113. |
|