Thomas Ferry, Maja Beck-Popovic, Nicolas Von der Weid, S Pernet Fattet, I Felberbaum.
Department medico-chirurgical de pediatrie, Lausanne, Switzerland.
ADDRESS FOR CORRESPONDENCE
Dr Thomas Ferry, CHUV, Bugnon 46, CH-1011, Lausanne. Department medico-chirurgical de pediatrie, Switzerland.
Email: Thomas.Ferry@chuv.ch | | Abstract | | Many children complain of back pain. We report on a 7 year old child who presented with persistent back pain and weakness. On physical examination, the child look tired, pale, without neurological deficit. Standard X-ray and CT of the spine showed multiple compressive fractures. Laboratory analyses revealed hypercalcemia, hyperuricemia, elevated LDH, and discrete thrombocytopenia with otherwise normal hemoglobin and white blood cell. Bone marrow aspiration and biopsy revealed a hypercellular bone marrow infiltrate to 95% by small round blue cells. The cells were negative for Langerhans cell histiocytosis or for leukemia, but positive for markers of rhabdomyosarcoma. The alveolar type was confirmed by cytogenetics. | | | | Introduction | Rhabdomyosarcoma (RMS) is a soft tissue neoplasm that occurs in children and rarely in adults. It accounts for 50 percent of malignant soft tissue sarcomas (1). On the other side, back pain in school children is common with a cumulative incidence of about 27% percent, the majority of these are self-limiting and the children uncommonly go to the paediatrician (2).
| | | | Case Report | A 7 year-old child presented an 8-week history of back pain. She experienced two traumas during these 8 weeks, one at the beginning with a fall during a trampoline session and the other two weeks later as a fall on the stairs. She began to complain of back pain after the first trauma which increased progressively and occurred even at night in spite of appropriate analgesia with paracetamol and ibuprofen. After some days, she developed weakness of the lower limb with secondary difficulty to walk. At this stage, she saw her paediatrician who referred to hospital for investigations. On physical examination, the child looked tired, pale, was slightly dehydrated and suffered intense back pain. Except from the weakness of the lower limb, no other neurological deficit was found. Standard X-ray and CT of the spine (Figure 1) showed compressive fractures of T4-T6-T7-T8-T11-L1-L4 and modification of the bone structure suggesting an underlying disease. Blood analyses revealed a slight thrombocytopenia of 1,43,000/cu mm with otherwise a normal hemoglobin of 13.0 g/L and WBC of 13,300/cu mm (57% neutrophil, 33% lymphocyte, 9% monocyte, 1% eosinophil); a slightly elevated sedimentation rate at 38 mm/h, a normal CRP of 3 mg/L, and hypercalcemia of 3,13 mmol/L (N: 2,15-2,55) with slightly elevated ionized Calcium of 1,58 mmol/L (N:1,10-1,50), slightly elevated uric acid of 375 mol/L (N: 111-353), hyperferritinemia of 429 mol/L (N: 10-160) and high LDH 1010 U/L (N: 155-345). PTH and PTHrp were very low at < 2,5 ng/L and < 0,3 pmol/L respectively and 25-OH Vit D3 21,5 mcg/L was normal. At this stage, a differential diagnosis between histiocytosis and leukaemia was considered and the child was referred to our oncology unit for further investigation.
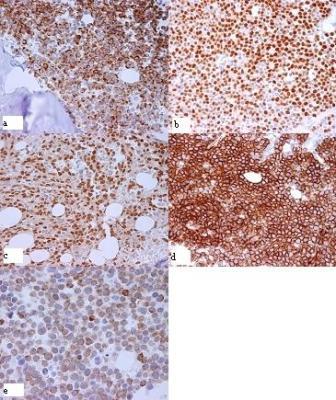
Bone marrow aspiration and biopsy were performed revealing a hypercellular bone marrow infiltrated to 95% by small round blue cells. Surprisingly the cells were negative for leukemia or Langerhans cell histiocytosis, but positive for markers of RMS (Figure 2). Cytogenetic analysis confirmed the alveolar type with the fusion complex PAX3-FKHR and t(2;13) translocation. A bone scan was performed showing diffuse enhancement of the skeleton and both kidneys. Thoraco-abdominal CT-scan fail to find the initial lesion. Repeated clinical examination revealed finally a small subcutaneous nodule at the postero-lateral side of the left arm (9x7mm). Magnetic resonance and biopsy confirmed the initial lesion of RMS.
This young girl also presented an acute renal failure with tubulopathy secondary to the renal parenchymatous infiltration of the tumoral cells and contrast injection for CT-scan, which resolved after introduction of the chemotherapy with vincristine, dactinomycin, cyclophosphamide. Dialysis was not required.
Figure 1. a) Initial standard X-ray of the spine showing multiple compressive fractures. b) and c) CT-scan confirming the fractures at T4-6-7-8-11-L1. d) T2-IRM showing T11 fracture with protrusion into the spinal thoracic canal
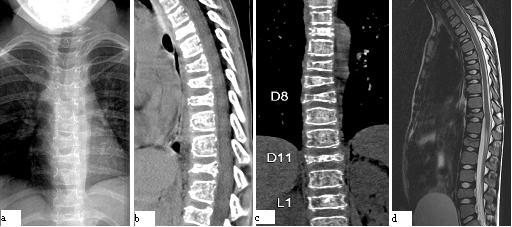
Figure 2:
 | | | | Discussion | Back pain is unusual in young children, but it becomes more common on rising age (2). Among children consulting for back pain, 50% will present an underlying disease (3). In younger children, especially under the age of 4, persistent back pain always needs investigations according to the 50% having a specific or serious cause beneath. Differential diagnosis includes musculoskeletal (trauma/fractures, spondylosis/spondylolisthesis, Scheuermann's disease, juvenile intervertebral disc calcification, disc herniation, congenital spinal anomalies/scoliosis, aneurysmal bone cyst, sacroiliac joint stress reaction, non-specific back pain), inflammatory (ankylosing spondylitis, Reiter syndrome), neoplastic (osteoid osteoma, leukaemia, neurofibroma, histiocytosis, osteosarcoma), infectious diseases (discitis/vertebral osteomyelitis, epidural abscess, pyelonephritis, pelvic inflammatory disease, pneumonia, viral myalgia). Alarming symptoms like progressive pain with worsening, associated neurological anomalies, bowel or bladder symptoms, age < 4 years, duration > 4 weeks, systemic features like fever - loss of weight - apathy, night pain, acute trauma, must push to further investigations.
RMS is the most common soft tissue tumor of childhood, since it accounts for one-half of all soft tissue sarcoma and 3 to 4 percent of all paediatric cancers (1). It arises anywhere in the body, most frequently in the head and neck in young children, and in the extremities in adolescents. Histologically RMS can be confused with small round blue cell tumors of childhood such as lymphoma/leukemia, osteosarcoma, Ewing's sarcoma and chondrosarcoma. In our patient, bone marrow morphology suggested acute leukemia. Normal complete blood cell count and hypercalcemia opened differential diagnosis to RMS, confirmed by immunohistochemical and molecular analysis.
The pathophysiology of hypercalcemia in neoplasm seems to be related to two different mechanisms, the first one being bone destruction by osteolytic metastases (more frequent) and the second one being bone resorption produced by PTH or PTHrp released by tumors (4). In childhood, hypercalcemia is rare and is usually related to leukaemia (5-9), and, in some cases, to solid tumors (neuroblastoma, RMS, lymphoma). In our case, hypercalcemia was secondary to the extensive osteolytic metastases. It was treated with overhydration, furosemide and pamidronate during several days.
Molecular abnormalities of alveolar RMS consist of mainly 2 chromosomal translocations. The fusion-gene PAX3-FKHR with (2;13)(q35;q14) is the more common (55%) abnormality found in alveolar type; the second, the fusion-gene PAX7-FKHR t(1;13)(p36;q14) is less common (22%), occurs usually in younger children with predominantly but not exclusive extremity lesion and a better outcome (10-11). The initial lesion in this case, however, with PAX3-FKHR is, surprisingly, located in an extremity.
This atypical presentation is very rare. A few similar cases in the literature have been described. Shinkoda and al. mentioned three cases of RMS miming acute leukaemia (12). Sandberg A. and al. (13) mentioned one case of a 12-year-old child mimicking lymphoblastic acute leukaemia and Etcubanas E. and al. (14) reported on 10 cases, the referring diagnosis was for 5 patients an acute leukaemia, 3 patients a disseminated malignancy, one patient an histiocytic lymphoma and one patient an osteosarcoma. For 6 patients, diagnosis of RMS was made by bone marrow aspirate or lymph node biopsy. For the other four patients, two patients had an initial misdiagnosis of neuroblastoma on bone marrow biopsy, one patient had histiocytic lymphoma on bone marrow aspirate and one had a metastatic sarcoma on bone marrow aspirate. Only 4 patients had a primary lesion being found retrospectively. Okcu et al described another 3 cases (15), all presenting the initial diagnosis of acute leukaemia. Other similar cases have been reported (16-19). | | | | Conclusion | | In conclusion, diffuse bone marrow RMS can be confused with acute leukaemia. Our case combines the rare features of back pain as initial presentation of a systemic disease with leukaemia-like bone marrow infiltration and is an uncommon, rarely reported clinical presentation of RMS. Back pain in children must always be taken seriously and properly investigated. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Ries LAG, Harkins D, Krapcho M, Mariotto A, Miller BA, Feuer EJ, et al (eds). SEER Cancer Statistics Review, 1975-2003, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2003/, based on November 2005 SEER data submission, posted to the SEER web site, 2006. Leah J.Jeffries and al, Spine vol 32, number 23, 2630-2637.
- Hollingworth P. Back pain in children. Br J Rheumatol. 1996; 35: 1022-1028. [CrossRef]
- Elomaa I, Lehto VP, Selander RK. Hypercalcemia and elevated serum parathyroid hormone level in association with rhabdomyosarcoma. Arch Pathol Lab Med. 1984; 108: 701-703. [PubMed]
- McKay C, Furman WL. Hypercalcemia complicating childhood malignancies. Cancer. 1993; 72: 256-260. [CrossRef]
- Harguindey S, DeCastro L, Barcos M, Getaz EP, Henderson ES, Freeman A. Hypercalcemia complicating childhood malignancies: a report of seven cases with some pathophysiological considerations. Cancer.1979; 44: 2280-2290. [CrossRef]
- Hazani A, Tatarsky I. Hypercalcemia, warning signal of acute leukemia. Nouv Rev Fr Hematol. 1972; 12: 259-266. [PubMed]
- Jordan GW. Serum calcium and phosphorus abnormalities in leukemia. Am J Med. 1966; 41: 381-390. [CrossRef]
- Hutchinson RJ, Shapiro SA, Raney RB Jr. Elevated parathyroid hormone levels in association with rhabdomyosarcoma. J Pediatr. 1978; 92: 780-781. [CrossRef]
- Sorensen PH, Lynch JC, Qualman SJ, Tirabosco R, Lim JF, Maurer HM, et al. PAX3-FKHR and PAX7-FKHR gene fusions are prognostic indicators in alveolar rhabdomyosarcoma: a report from the children's oncology group. J Clin Oncol. 2002; 20: 2672-2679. [CrossRef]
- Kazanowska B, Reich A, Stegmaier S, Bekassy AN, Leuschner I, Chybicka A, Koscielniak E. Pax3-fkhr and pax7-fkhr fusion genes impact outcome of alveolar rhabdomyosarcoma in children. Fetal Pediatr Pathol. 2007; 26: 17-31. [CrossRef]
- Shinkoda Y, Nagatoshi Y, Fukano R, Nishiyama K, Okamura J. Rhabdomyosarcoma masquerading as acute leukemia. Pediatr Blood Cancer. 2009; 52: 286-287. [CrossRef]
- Sandberg AA, Stone JF, Czarnecki L, Cohen JD. Hematologic masquerade of rhabdomyosarcoma. Am J Hematol. 2001; 68: 51-57. [CrossRef]
- Etcubanas E, Peiper S, Stass S, Green A. Rhabdomyosarcoma, presenting as disseminated malignancy from an unknown primary site: a retrospective study of ten pediatric cases. Med Pediatr Oncol. 1989; 17:39-44. [CrossRef]
- Okcu MF, Hicks J, Horowitz M. Rhabdomyosarcoma and undifferentiated sarcoma in childhood and adolescence. Available at URL: http://www.uptodate.com/patients/content/topic.do?topicKey=~PciiJzHU1Gv1gc. Accessed on 1st June 2010.
- Lisboa S, Cerveira N, Vieira J, Torres L, Ferreira AM, Afonso M, et al. Genetic diagnosis of alveolar rhabdomyosarcoma in the bone marrow of a patient without evidence of primary tumor. Pediatr Blood Cancer. 2008; 51: 554-557. [CrossRef]
- Hanke CA, Roessler J, Stegmaier S, Koscielniak E, Niemeyer CM, Kontny U. Alveolar rhabdomyosarcoma mimicking lymphoma with bone marrow involvement. Eur J Pediatr. 2007; 166: 505-506. [CrossRef]
- Yamaguchi K, Koga Y, Suminoe A, Saito Y, Matsuzaki A, Kanno S, et al. Alveolar rhabdomyosarcoma of unknown origin mimicking acute leukemia at the initial presentation. Rinsho Ketsueki. 2007; 48: 315-320. [PubMed]
- Srinivas U, Pillai L, Kar R, Mahapatra M, Gujra S, Pati HP. A case of rhabdomyosarcoma masquerading as acute leukemia at presentation: a case report. Indian J Pathol Microbiol. 2007; 50: 917-919. [PubMed]
|
| Cite this article as: | | Ferry T, Beck-Popovic M, Weid N V d, Fattet S P, Felberbaum I. FROM INITIAL COMMON BACK PAIN IN A CHILD TO FINAL DIFFUSE METASTATIC RHABDOMYOSARCOMA. Pediatr Oncall J. 2011;8: 13-15. |
|