Hiren N. Doshi, Kshitij Sheth, N C Joshi.
Blessed Teresa Advanced Pediatric Center,Dr. Balabhai Nanavati Hospital, Vile Parle, Mumbai, India.
ADDRESS FOR CORRESPONDENCE
Dr Hiren N Doshi, Consultant Pediatric Intensivist and Neonatologist, Blessed Teresa Advanced Pediatric Center, Dr. Balabhai Nanavati Hospital, Vile Parle (E), Mumbai.
Email: drhiren@msn.com. | | Abstract | Most critically ill children require intensive care to restore their abnormal hemodynamics back to normal. Sedation forms a major part of patient management. For long time sedation is monitored using clinical scores which are subjective, intermittent and time consuming. The aim of this study is to compare clinical score (COMFORT score) with Bispectral Index Score (BIS), which is objective, continuous and easy to interpret, in order to validate the use of BIS in PICU.
The study was a blinded, prospective one carried out in a level 3 PICU in Mumbai. Thirty three patients requiring mechanical ventilation along with sedation, for various pathologies were enrolled. Patients having neurological pathology were excluded. Simultaneous BIS and COMFORT scores were obtained while patient was on sedation, and also 2 hours after stopping sedation. Of the 33 patients evaluated, minimum age was 2 months and maximum 18 years with mean age of 5.19 years. The BIS scores correlated well with COMFORT scores in all age groups except for in children less than 1 year. BIS scores were more reliable with deeper levels of sedation and showed inaccuracies when the children were fully awake. This observation has little clinical significance as the need for assessment is obviously absent when the child is fully alert. Thus, BIS provides a real-time, continuous, objective, simple and reliable quantitative measurement of the changes in the consciousness level of sedated as well as paralyzed patients on mechanical ventilators. | | | | Keywords | | Bispectral index (BIS), sedation, COMFORT score, PICU, neurological monitoring | | | | Introduction | As pediatric intensive care comes of age, more and more attention is being paid on sedation, analgesia and anxiolysis in sick children. This inadvertently leads to an increased use of drugs which have a potential to cause hemodynamic instability and respiratory depression. There is always the potential to either under-sedate and cause stress and pain related morbidity or to over-sedate and cause unwanted respiratory interventions or risk hypoxic consequences.
Till recently, clinical parameters were the only means to judge level of sedation and were wrought with many limitations. It is time consuming, tedious, and operator dependant. Also, it is not possible to keep a continuous check on the level of sedation. Moreover, in children on neuromuscular blockade, the clinical method will obviously not be applicable. Only a few clinical scores have been validated for estimating the level of sedation in paediatric ICU patients. The best evaluated score is the COMFORT score developed by Ambuel et al in 1992. (1)
Validation of Bispectral Index score (BIS) to monitor depth of sedation in the pediatric age group in a PICU setting was the aim of this study. It was conducted in a level 3 PICU in a private trust hospital in Mumbai, India, which is equipped with BIS monitoring facility in each of its PICU bed. BIS scores were obtained and simultaneous clinically COMFORT scores were calculated and the two were compared using standard statistical methods. | | | | Methods & Materials | This prospective study was carried out in children between 2 months to 18 years requiring mechanical ventilation and receiving sedatives as per standard PICU protocols during the period from June 2007 to May 2009. Patients with neurological pathology, seizures, terminal illness (renal failure, brain death) were excluded as these conditions have confounding effect on electrical activity of brain. Permission was sought from the Hospital ethics committee and an informed consent was obtained from the parents.
The COMFORT score consists of eight categories and can evaluate a child's behaviour and physiological responses to discomfort, fear and pain in approximately 2 minutes. The COMFORT score is age independent because age-adapted physiological parameters are used. Apart from the examination of muscular tone, calculation of the COMFORT score does not require any stimulation of the patient. The COMFORT score can be divided into three groups. A score of 8-16 points corresponds to deep sedation, 17-26 indicates light sedation and 27-40 indicates inadequate sedation (2).
We studied 37 paediatric patients admitted to our PICU. After enrolment 4 patients were excluded since impedances did not comply with the quality requirements of the manufacturer (< 10 k Ohm
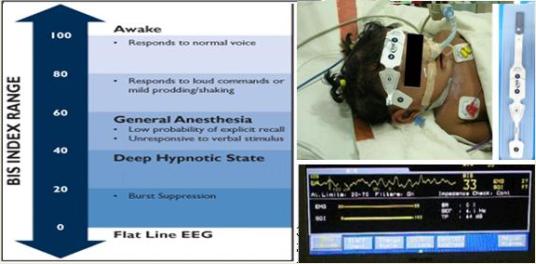
, signal quality index > 80), or recording could not be repeated at least twice. After PICU admission, the study was started when all examinations on admission were completed and all sources of irritation were eliminated. Electrodes were placed at F7, F8 and Fp (reference), and one electrode was placed beside Fp (ground) in accordance with the international ten-twenty system as proposed by Electrode Position Nomenclature Committee in 1991 (3). (Figure 1) Electrode sites were abraded using conventional alcohol swabs. Paediatric silver-silver-chloride self-adhesive EEG electrodes were applied (Aspect Sensor PaediatricTM MA, USA, for children < 5 years and Aspect Sensor Quarto MA, USA, for children > 5 years). An Aspect A-1000 TM monitor (software version 3.12; Aspect Medical Systems, Natick, MA, USA) was used to compute the BIS. As proposed by Triltsch AE, et al (4) in 2005, we included data wherein the impedance was < 5 Ohm. We also took into account the Signal Quality Index (SQI) which as proposed by the manufacturer to be more than 80. This ensured good quality data.
Once the child was intubated and started with sedation, BIS scores were obtained 2 hours after starting the sedation. Simultaneously, COMFORT score was also obtained. To avoid observer bias two different individuals obtained the scores separately. Five such readings were taken along with the SQI and impedance at an interval of 15 minutes. The reading of BIS with best SQI was selected along with simultaneous COMFORT score. To avoid bias by repeating analysis of data from the same patient, each patient was included only once in the statistical analysis. Second set of reading for the purpose of study was taken after one hour of stopping the sedation. This would help in identifying increase in BIS score with reducing levels of sedatives.
Statistical Analysis:
Non-Parametric correlation between BIS and COMFORT score on sedation and after stopping sedation was done using Spearman's Rho. Comparison of age specific, sex-specific, disease specific, sedation specific BIS and COMFORT scores were done using 1-way ANOVA.
Fig 1: The BIS Scale and the application of BIS electrodes with monitor screen grab
| | | | Results | The mean BIS scores on sedation was 34.6 + 9.7 with simultaneous mean COMFORT score of 12.5 + 1.8. The minimum BIS score on sedation recorded in the study was 15 and a maximum of 57 whereas minimum COMFORT score on sedation was 8 and a maximum of 17. Two hours after stopping the sedation, mean BIS score was 83.4 + 6.5 while the mean COMFORT score was 30.1 + 2.7. The minimum BIS score was 65 and maximum of 94. At the same time minimum and maximum COMFORT score were 21 and 36 respectively. We compared BIS and COMFORT score on sedation, the difference was statistically significant (p=0.026). This indicated that BIS correlated better with COMFORT score at deeper levels of sedation. However, when we compared BIS scores and COMFORT scores two hours after stopping sedation, there was no significant correlation.
Four children were below 1 year age group (12.1%), 17 children were in age group of 1-5 years (51.5%), and 12 children were aged > 5 years (36.4%). In the age group < 1 year, mean BIS on sedation was 25 while simultaneous COMFORT score was 11. Similarly for 1-5 years, simultaneous BIS and COMFORT were 33 and 83 respectively and in > 5 years age group it was 40 and 84 respectively. There was statistically significant difference in p-value (0.01) for children aged less than 1 year. This indicates that BIS values at age less than 1 year is less reliable than that at other ages. | | | | Discussion | The aim of this cross-sectional, blinded study was to determine whether BIS is a useful tool for assessing the level of sedation in critically ill pediatrics patients. For statistical calculation only one data set (BIS versus COMFORT score) per patient was evaluated. Therefore, bias introduced by including multiple observations from one patient was avoided. We compared BIS with COMFORT because it is the only scoring system validated for use in pediatric age-group (1).
The study showed significant correlation between BIS and COMFORT when child was on sedation. However, the correlation was not significant after stopping sedation. This indicated that at higher levels of consciousness, the BIS did not correlate well with COMFORT, but as level of sedation was increased, the two correlated well. This difference could be because of the movement artifacts contributed to the lower coefficient of determination for lighter sedated children than for children under deeper sedation. Similar findings were reported in adult settings by Nasraway SA Jr, et al (5) in 2002. In that study they had compared BIS score with SAS in 20 adult subjects and had concluded that excessive muscle movement by the patient is an important and spurious influence on BIS values. Also a review of literature on MEDLINE by Dominguez TE, et al (6) in 2006, concluded that Bispectral values correlate fairly well with commonly used clinical sedation scores, but more variability in the scores has been observed at lighter levels of sedation. Also, Bruhn et al (7), found similar results and concluded that electromyographic activity falsely elevates the Bispectral index.
Age-related BIS values have been a matter of debate. In our study, we found that BIS values were less predictive of level of sedation in children < 1 year. Similar results were shown by Davidson et al (8), wherein they compared BIS with the corresponding consciousness level during emergence from anesthesia in a prospective, blinded manner in children (
> 1 year old ) and infants ( < 1 year old ) undergoing elective circumcision. BIS increased significantly as sevoflurane concentrations decreased in children, but a similar relationship was not demonstrated in infants. Again Davidson et al (9), compared BIS and entropy in monitoring level of sedation in various age groups. Here again they found that in infants BIS was less reliable tool to assess depth of sedation. This finding may imply that the inability of EEG monitoring to predict awakening in small children is more a function of the nature of their arousal and consciousness rather than inherent changes in the EEG with maturation. It has been reported previously by Werry et al in 1996 that infants have an abrupt transition from unconsciousness or deep sedation, to arousal, thus suggesting a possibly more binary nature to their consciousness. (10) | | | | Conclusion | BIS correlates well with COMFORT scores in pediatric patients above 1 year of age. BIS scores are very accurate with deeper levels of sedation and start showing inaccuracies as level of consciousness improves, probably due to interference from EMG signals. Even though both BIS and COMFORT scores correlate well; BIS being objective, direct and continuous assessment of effect of sedative drugs on brain, it helps intensivist better, than time consuming, indirect subjective clinical scores. Also, in patients receiving neuromuscular blocking agents, it is impossible to assess sedation using clinical scores like COMFORT score. It is here that objective assessment using BIS is very important. Finally, the complications using BIS are minimal and not at all life threatening, making it a safe tool to use.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Ambuel B, Hamlett KW, Marx CM, Blumer JL. Assessing distress in paediatric intensive care environments: the COMFORT scale. J Pediatr Psychol. 1992; 17: 95-109. [CrossRef]
- Marx CM, Smith PG, Lowrie LH, Hamlett KW, Ambuel B, Yamashita TS, et al. Optimal sedation of mechanically ventilated paediatric critical care patients. Crit Care Med. 1994; 22: 163-170. [CrossRef]
- American Electroencephalographic Society guidelines for standard electrode position nomenclature. J Clin Neurophysiol. 1991; 8: 200-202. [CrossRef]
- Triltsch AE, Nestmann G, Orawa H, Moshirzadeh M, Sander M, Grobe J, et al. Bispectral index versus COMFORT score to determine the level of sedation in paediatric intensive care unit patients: a prospective study. Crit Care. 2005; 9: R9-17. [CrossRef]
- Nasraway SA SA Jr, Wu EC, Kelleher RM, Yasuda CM, Donnelly AM. How reliable is the Bispectral index in critically ill patients- A prospective, comparative, single-blinded observer study. Crit Care Med. 2002; 30: 1483-1487. [CrossRef]
- Dominguez TE, Helfaer MA. Review of Bispectral Index Monitoring in the Emergency Department and Paediatric Intensive Care Unit. Pediatr Emerg Care. 2006; 22: 815-821. [CrossRef]
- Bruhn J, Bouillon TW, Shafer SL. Electromyographic activity falsely elevates the Bispectral index. Anesthesiology. 2000; 92: 1485-1487. [CrossRef]
- Davidson AJ, McCann ME, Devavaram P, Auble SA, Sullivan LJ, Gillis JM, et al. The differences in Bispectral index between infants and children during emergence from anesthesia after circumcision surgery. Anesth Analg. 2001; 93: 326-330. [CrossRef]
- Davidson AJ, Huang GH, Rebmann CS and Ellery C. Performance of entropy and Bispectral Index as measures of anaesthesia effect in children of different ages. Br J Anaesth. 2005; 95: 674-679. [CrossRef]
- Werry C, Neulinger A, Eckert O, Lehmkuhl P, Pichlmayr I. Age-related correlation between EEG parameters and depth of anesthesia under propofol. Effect of fentanyl. Anaesthesist. 1996; 45: 722-730. [CrossRef]
|
| Cite this article as: | | Doshi H N, Sheth K, Joshi N C. Comparing Bispectral Index Score to COMFORT Score in assessing sedation in Pediatric patients. Pediatr Oncall J. 2011;8: 31-33. |
|