Amit Agrawal, Rashmi Agrawal.
Department of Pediatrics, Chirayu Medical College and Hospital, Bairagarh, Bhopal, MP, India.
ADDRESS FOR CORRESPONDENCE
Dr Amit Agrawal, 28, Ravidas Nagar, Near Nizamuddin Colony, Indrapuri, Bhopal. India.
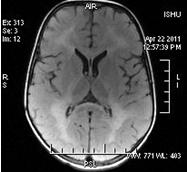
Email: agrawaldramit@yahoo.co.in | | Keywords | | Pelizaeus-Merzbacher disease, dysmyelination, leukodystrophy | | | A 3-year-old male was presented with complaints of delayed milestones, language impairment, gradually increasing spasticity, difficulty in swallowing, and abnormal movements. Patient was a product of non-consanguineous marriage, born by normal vaginal delivery with no significant antenatal, intranatal, and immediate postnatal events. Patient was the youngest of eight siblings, of which six female siblings were healthy, normal, and growing appropriately for age, but one male sibling died of similar complaints at around 5 years of age. Parents noticed some abnormal jerky movements of eyes starting from second month of life. His milestones were delayed and he was not able to support his head by the age 6 months and he never achieved sitting or standing without support but he was able to sit with support. He also had stridor, difficulty in swallowing, language impairment, and tonic-clonic convulsions and he was being managed with a diagnosis of cerebral palsy and was referred to our centre for further management. On detailed physical and neurological examination, patient was having pendular nystagmus, stridor, spastic quadriparesis, hyper-reflexia, and positive Babinski sign. Palatal and gag reflexes were weak with some difficulty in swallowing and global developmental delay. During hospital stay, he had 2 episodes of tonic-clonic convulsions which subsided with antiepileptics. His routine haematological investigations and chest X-ray were within normal limits. Auditory and visual evoked potentials were normal. MRI brain imaging revealed diffuse and symmetric T2 and flair high signal intensity throughout the bilateral cerebral white matter, genu of corpus callosum and subcortical U fibres along with tigroid pattern within the corona radiate (Figures 1-2). On the basis of these clinical and imaging findings diagnosis of Pelizaeus-Merzbacher disease (PMD) was made and treatment with antiepileptics, antispastic medications, and physiotherapy was started to reduce spasticity and convulsions.
Fig.1 - T2-weighted image showing diffuse hyperintensity throughout cerebral white matter.
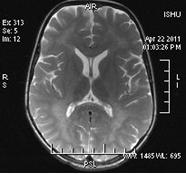
Fig.2 - Flair image showing hyperintensity involving bilateral cerebral white matter, corpus callosum, and subcortical U fibres.
Pelizaeus-Merzbacher disease (PMD), a rare dysmyelinating disorder affecting white matter, was first described by Pelizaeus in 1885 and Merzbacher in 1910. (1) Clinical presentation of PMD varies widely, depending primarily on the nature of causative mutation, and to a certain extent, on other genetic and environmental influences. (2) PMD is a dysmyelinating leukodystrophy in contrast to other leukodystrophies like metachromatic leukodystrophy, adrenoleukodystrophy and multiple sclerosis, which are demyelinating disorders. In demyelinating disorders, myelin is formed, deposited around the axons and then destroyed later; while in dysmyelinating disorders normal myelination does not occur. (3) Most of the PMD cases have an identifiable mutation in PLP1 containing region of the X chromosome (Xq22), which could be duplications (60-70%), or point mutations resulting in base substitutions, insertions, or deletions (15-20%). This region encodes a major central nervous system (CNS) myelin protein, PLP1, which constitutes about 50% of the white matter mass, and is abundantly expressed in oligodendrocytes. (4) PMD typically affects males but sometimes female heterozygotes can be clinically affected, especially those who carry alleles that are relatively mild in males, as these mutations do not cause apoptosis of the affected oligodendrocytes. In this case also elder male sibling died of same disease at the age of about 5 years while other six female siblings were normal, supporting the possibility of X-inked recessive disorder.
Classic PMD usually presents with infantile-onset nystagmus, weakness, developmental delay followed by development of ataxia, spasticity, involuntary movements, and cognitive delay. Most patients never ambulate, although some language skills may be acquired and survival into the sixth decade is not unusual. On the opposite end, the more severe variant connatal PMD presents in neonatal period or early infancy. It is characterized by nystagmus beginning within the first week or two of life, stridor, respiratory difficulty, and hypotonia. Sometimes, hypotonia may be severe enough to be misdiagnosed as spinal muscular atrophy, however severe spasticity later replaces hypotonia. These patients also have failure to thrive, significantly delayed motor milestones, limited language skills, even seizures and death often occurs during the first decade of life, typically due to respiratory complications. (4,5) Our case was also being treated as spastic cerebral palsy for a long time which finally diagnosed as a case of PMD on brain MRI study as also reported previously. (6) MRI, the most useful imaging study, can demonstrate symmetric and widespread abnormality of the white matter of cerebrum, brain stem, and cerebellum, typically evident as hyperintensity on T2-weighted and hypointensity on T1-weighted images, which can be either diffuse or patchy. Additionally, the absolute volume of white matter can also be reduced, especially in connatal PMD. (7) Definitive diagnosis can only be made by molecular testing by detecting PLP1 gene mutations.
Presently, there is no specific treatment for PMD and treatment is limited to supportive care including physiotherapy and antispasticity medications including intrathecal baclofen. Correct posture and seating can help minimize joint contractures, dislocations, and kyphoscoliosis. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Boespflug-Tanguy O, Mimault C, Melki J, Cavagna A, Giraud G, Pham Dinh D, et al. Genetic Homogeneity of Pelizaeus-Merzbacher Disease: Tight Linkage to the Proteolipoprotein Locus in 16 Affected Families. Am J Hum Genet. 1994;55:461-467. [PubMed] [PMC free article]
- Woodward KJ. The molecular and cellular defects underlying Pelizaeus-Merzbacher disease. Expert Rev Mol Med. 2008;19:e14. [CrossRef]
- Takanashi J, Sugita K, Tanabe Y, Nagasawa K, Inoue K, Osaka H, et al. MR revealed myelination in the cerebral corticospinal tract as a marker for Pelizaeus-Merzbacher's disease with proteolipid protein gene duplication. AJNR Am J Neuroradiol. 1999; 20: 1822-1828. [PubMed]
- Koeppen AH, Robitaille Y. Pelizaeus-Merzbacher disease. J Neuropathol Exp Neurol. 2002; 61: 747-759. [CrossRef]
- Beri S, Hussain N, Gosalakkal JA. Connatal Pelizaeus-Merzbacher Disease: A Great Masquerader. Indian J Pediatr. 2010;77:338. [CrossRef]
- Caord Artal J, Prats Vinas JM, Garaizar Axpe C, Zuazo Zamalloa E. Congenital Pelizaeus-Merzbacher disease simulating infantile spastic cerebral palsy. Neurologia 1995; 10: 57-58.
- Jasek F, Chateil JF, Fontan D, Diard F, Desforges J. Pelizaeus-Merzbacher disease: the diagnostic contribution of MRI. Arch Fr Pediatr. 1990;47:265-269. [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2012.50
|
| Cite this article as: | | Agrawal A, Agrawal R. DON`T JUST LABEL AS CEREBRAL PALSY, IT COULD BE PELIZAEUS-MERZBACHER DISEASE. Pediatr Oncall J. 2012;9: 78-80. doi: 10.7199/ped.oncall.2012.50 |
|