Sara S Dhanawade1, Subodh M Dhanawade2.
1Department of Paediatrics, Bharati Vidyapeeth Deemed University Medical College and Hospital, Sangli, Maharashtra, India,
2Consultant Cardiologist, Wanless Hospital, Miraj, Sangli, Maharashtra, India.
ADDRESS FOR CORRESPONDENCE
Sara S Dhanawade, Department of Paediatrics, Bharati Vidyapeeth Deemed University Medical College & Hospital, Sangli, Maharashtra, India 416414.
Email: sarasubodh@yahoo.com | | Keywords | | Intracranial mycotic aneurysm, infective endocarditis | | | A 12 years old boy presented with prolonged fever of one year duration. He was known to have bicuspid aortic valve with aortic stenosis. He had 3 prior hospitalizations elsewhere for persistent fever and had received multiple antibiotics. The echocardiographic examination on 2 occasions during this period did not reveal any vegetation. On examination he was febrile, pale, tachycardic and had grade 2 finger clubbing. Systemic examination revealed grade 3/6 ejection systolic murmur and an early diastolic murmur in the aortic area and hepatosplenomegaly. Investigations revealed hemoglobin of 8g /dl, total leucocyte count of 2700/cumm, platelet count of 87500/cumm and ESR of 75mm. There was microscopic hematuria, albuminuria and granular casts. Cardiac evaluation revealed cardiomegaly and left ventricular hypertrophy. Echocardiography revealed large vegetations on the aortic valve with moderate aortic regurgitation. On ultrasonography hepatosplenomegaly and bilateral enlarged kidneys with poor corticomedullary differentiation was noted. Serial blood cultures were sterile. He was started on ceftazidime and vancomycin. On the 3rd hospital day he suddenly developed headache, vomiting, generalized seizures with altered sensorium. He had signs of raised intracranial tension but no meningeal signs or focal neurological deficit. CT scan revealed intracerebral bleed in the right parieto-occipital region with extension into the ventricles. (Fig.1) He was started on anticonvulsants, low dose mannitol and dexamethasone. There was improvement in the sensorium within 24 hours and convulsions were controlled. CT angiography disclosed a small aneurysm of 3 mm involving the parietal branch of right middle cerebral artery suggestive of mycotic aneurysm. (Fig.2) He was managed conservatively with intravenous antibiotics for 6 weeks. CT angiography repeated at 2months showed complete resolution of the aneurysm. Echocardiography repeated revealed persistence of vegetation and severe aortic regurgitation. As the patient started having signs of cardiac decompensation he was referred to higher center for cardiac surgery.
Figure 1 : CT head showing intracerebral bleed in the right parieto-occipital region with extension into the ventricles
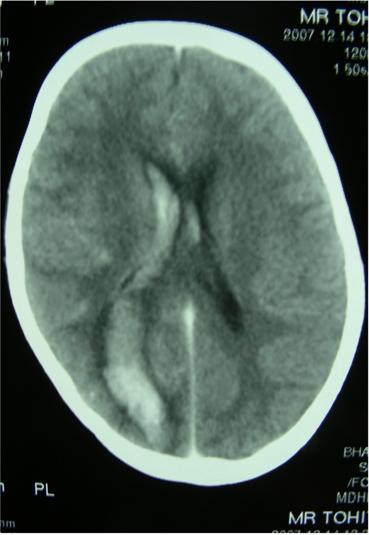
Figure 2 : CT angiography showing a small aneurysm of 3 mm involving the parietal branch of right middle cerebral artery suggestive of mycotic aneurysm

Infective endocarditis (IE) and neurological manifestation is a clinically important association seen in 20-40% of patients. Intracranial mycotic aneurysm (MA) occurs in about 2-10% of them. Most of the mycotic aneurysms remain asymptomatic with only about 1.7% rupture. (1) The fatality rate of ruptured MA was reported to be 80% in earlier studies and 10-32% in recent reports. (2) Left sided endocarditis and presence of highly virulent organism like staphylococcus aureus are considered risk factors for development of neurological complications. (3) MA are more common but develop at a later stage of the disease in subacute endocarditis whereas aneurysm formation though less common occur early in acute endocarditis. (2) The risk of rupture of MA is highest early in the course of the disease and appropriate antibiotic therapy tends to prevent its rupture. (4) This patient presented to us late with sub-acute endocarditis evolving over months making it difficult to establish the exact onset of IE. We presume he developed MA later in the course of the disease and the delayed institution of appropriate antibiotic therapy could have been a factor responsible for the bleed.
The management approach depends on whether the aneurysm had ruptured or not, presence of mass effect and the site. (3) Current recommendations regarding the management of MA have been divided into medical, endovascular and surgical therapies. They are known to resolve with medical therapy as was the case with our patient. (5) The recommended treatment is intravenous antibiotics for 4 to 6 weeks. A repeat angiography is required to confirm resolution. Endovascular coiling has now evolved as a popular modality of treatment option. Surgical interventions are reserved for definitive indications. (2) Surgical treatment with open craniotomy and aneurysm clipping or endovascular treatment should be considered in patients with multiple aneurysms, ruptured aneurysm with deepening coma and mass effect or aneurysm which enlarge while on medical therapy. (3)
Acknowledgments : Authors thank Dr. V. B. Borade, Dean, Bharati Vidyapeeth Deemed University Medical College & Hospital, Sangli. for permission to publish this manuscript.
Authors Contribution: SSD was involved in the management of the case. SMD did the cardiac evaluation. Both the authors were involved in the drafting of the paper. SSD will act as the guarantor.
Source of Funding: None
Competing Interests: None | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Karchmer AW. Infective Endocarditis: In Braunwald E, Zipes DP, Libby P, editors. Heart Disease: A Textbook of cardiovascular medicine. 6th edn. W.B Saunders Company; 2001. p.1723- 1748.
- Kong KH, Chan KF. Ruptured intracranial mycotic aneurysm: a rare cause of intracranial hemorrhage. Arch Phys Med Rehabil 1995; 76: 287-289. [CrossRef]
- Kannoth S, Thomas SV. Intracranial Microbial Aneurysm (infectious aneurysm): Current options for Diagnosis and Management. Neurocrit care 2009; 11: 120-129. [CrossRef]
- Tunkel AR, Kaye D. Neurologic complications of infective endocarditis. Neurol Clin 1993; 11: 419-440. [CrossRef]
- Patel FM, Das A, Banerjee AK. Neuropathological complications of infective endocarditis: study of autopsy material. Neurol India 2001; 49: 41-46. [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2013.8
|
| Cite this article as: | | Dhanawade S S, Dhanawade S M. RUPTURED INTRACRANIAL MYCOTIC ANEURYSM COMPLICATING INFECTIVE ENDOCARDITIS. Pediatr Oncall J. 2013;10: 23-24. doi: 10.7199/ped.oncall.2013.8 |
|