Rakhi Jain1, Sunil Taneja1, Ruchi Puri2, SS Rathore2.
1Department of Pediatrics, GSVM Medical College, Kanpur,
2Consultant Pediatrician, Madhuraj Hospital, Kanpur.
ADDRESS FOR CORRESPONDENCE
Dr Rakhi Jain, 98, Y1, Kidwai nagar, Kanpur, UP.
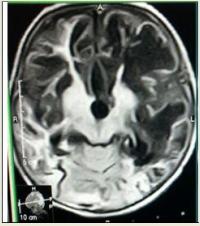
Email: drrakhi09@gmail.com | A six months old female child was admitted with fever and focal seizures for one day. On examination, vitals were stable but baby was in altered sensorium and had bulging anterior fontanelle. Focal seizures were refractory to phenobarbitone and phenytoin hence valproate and levetiracetam were used to control seizures. Intravenous antibiotics were started with provisional diagnosis of acute bacterial meningitis but cerebrospinal fluid (CSF) examination showed 90 cells/hpf of which 60% were lymphocytes and 40% polymorphs, glucose was 81 mg% and protein was 58mg% with 200 RBCs suggesting herpes simplex virus (HSV) infection. Injection acyclovir was started at the dose of 20 mg/kg/dose three times a day (60 mg/kg/day) but patient did not improve. Serology for HSV showed positive HSV (1+2) IgG and negative IgM. Hence acyclovir was stopped. CT brain was normal. Repeat CSF showed 50 WBCs/hpf with 30% polymorphs and 70% lymphocytes, 200 RBCs, sugar 45 mg% and protein 180 mg/dl. Real time PCR in CSF was positive for HSV 1. MRI brain showed left temporal encephalitis (Figure 1). acyclovir was restarted and given at the same dose for 21 days. Eye examination revealed chorioretinitis (Figure 2). Repeat MRI scan showed bilateral gyral edema with diffuse white matter hyperintensity in cerebral hemisphere. HIV 1 & 2 was non reactive and NMDA receptor antibody in serum was negative. Toxoplasma IgG was positive and IgM was negative while CMV IgG was positive & IgM was negative. MRI brain after one month showed extensive loss of brain substance in supratentorial region sparing bilateral occipital cortex with mild dilatation of bilateral lateral ventricles. (Figure 3)
Figure 1: MRI showing left temporal lobe Hypodensity on T1 weighted image
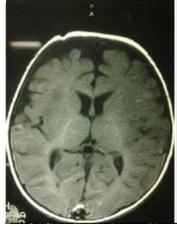
Figure 2: Chorioretinitis on fundoscopy
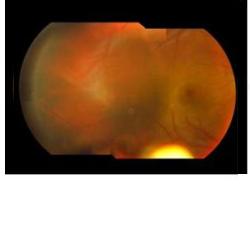
Figure 3: MRI showing extensive necrotizing sequelae
Viral encephalitis associated with chorioretinitis in an infant may be due to toxoplasmosis, syphilis, cytomegalic inclusion disease or others. (1) Yet, often the etiology remains obscure. (2) HSV is known to cause severe disease involving skin, eye, mouth, CNS or manifest disseminated infection involving multiple organ system especially in neonates which may present even in absence of skin lesions. Chances of neurological sequelae are high. (3,4,5) This case of HSV encephalitis shows necrotizing HSV infection leading to severe brain and retinal damage which may lead to sequelae in future. Mitchell et al (6) described an infant who suffered from recurrent herpes simplex infections of the skin in association with chorioretinitis and evidence of significant central nervous disease. Reports of chorioretinitis and cerebral disease accompanying a generalized cutaneous eruption of presumed herpetic etiology are also on record. (7) Cogan et al (8) suggest that the evolution of the ophthalmic findings clinically and the microscopic appearance of the retinal lesions are more consistent with an immunologic process than with direct invasion of the retinae by the virus. Treatment of HSV retinitis is acyclovir as for HSV encephalitis 60 mg/kg/dose thrice a day. (9) Untreated HSV retinitis may lead to scarring and blindness. Laser photocoagulation is seen to have some role in improving visual acuity. (9)
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Haymaker W, Girdany BR, Stephens J, Lillie RD, Fetterman GH. Cerebral involvement with advanced periventricular calcification in generalized cytomegalic inclusion disease in the newborn; a clinicopathological report of a case diagnosed during life. J Neuropathol Exp Neurol. 1954; 13: 562-586. [CrossRef] [PubMed]
- Sabin AB, Feldman HA. Chorioretinopathy Associated With Other Evidence of Cerebral Damage in Childhood: Syndrome of Unknown Etiology Separable From Congenital Toxoplasmosis. J Pediatr. 1949; 35: 296-309. [CrossRef]
- Lawrence C. Herpes simplex viruses. In: Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison's Principles of Internal Medicine. 17th ed. New York, NY: McGraw-Hill Professional; 2008: 2631.
- Hsieh WB, Chiu NC, Hu KC, Ho CS, Huang FY. Outcome of herpes simplex encephalitis in children. J Microbiol Immunol Infect. 2007; 40: 34-38. [PubMed]
- Kimberlin DW. Advances in the treatment of neonatal herpes simplex infections. Rev Med Virol. 2001; 11: 157-163. [CrossRef] [PubMed]
- Mitchell JE, McCall FC. Transplacental Infection by Herpes Simplex Virus. Amer J Dis Child. 1963; 106: 207-209. [PubMed]
- Florman AL, Mindlin RL. Generalized Herpes Simplex in an Eleven-Year-Old Premature Infant. Amer J Dis Child. 1952; 83: 481-486.
- Cogan DG, Kuwabara T, Young GF, Knox DL. Herpes Simplex Retinopathy in an Infant. Arch Ophthal. 1964; 72 : 641-645. [CrossRef] [PubMed]
- Tarkkanen A, Laatikainen L. Late ocular manifestations in neonatal herpes simplex infection. Br J Ophthalmol. 1977; 61: 608-616. [CrossRef] [PubMed] [PMC free article]
DOI: https://doi.org/10.7199/ped.oncall.2013.54
|
| Cite this article as: | | Jain R, Taneja S, Puri R, Rathore S. HSV Encephalitis Associated with Chorioretinitis. Pediatr Oncall J. 2013;10: 120-121. doi: 10.7199/ped.oncall.2013.54 |
|