Manoj Kumar Jangid1, Sunil Kumar Yadav2.
1Department of Pediatrics, IBN SINA Hospital, State of Kuwait,
2Department of Pediatric surgery, IBN SINA Hospital, State of Kuwait.
ADDRESS FOR CORRESPONDENCE
Dr Manoj Kumar Jangid, Department of Pediatric Surgery, IBN SINA Hospital, State of Kuwait.
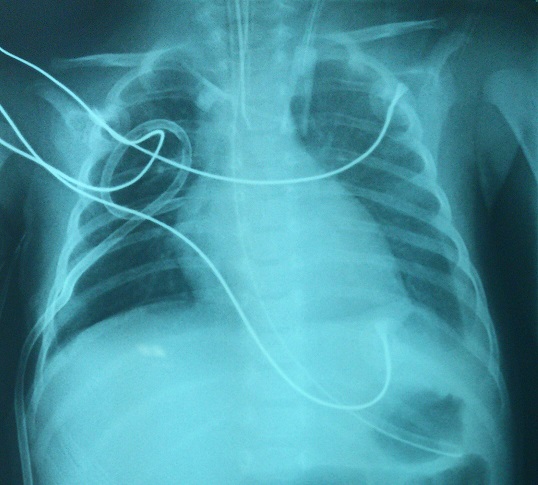
Email: drmanojjangid@gmail.com | | Keywords | | External jugular vein catheterization, pleural effusion, complications | | | | Abstract | | A variety of complications are known with external jugular vein catheterization and most of the times, the immediate complications are anticipated and managed; whereas, delayed complications can go unnoticed and sometimes may be quite serious as well. We encountered an unusual life threatening complication 2 days after right external jugular vein catheterization in a 2 month old infant in the form of acute respiratory distress due to development of right hydrothorax. The case highlights the importance of continued vigilance regarding the correct position and function of external jugular venous catheters so as to prevent serious complications. | | | | Introduction | | A number of well recognized complications are associated with internal jugular vein catheterization including bleeding, pneumo and hemothorax, chylothorax, air embolism, pericardial tamponade, infections, hematoma, nerve injuries and Horner’s syndrome. (1-4) However significant complications related to external jugular vein catheterization are uncommon. We report a case of massive infusion hydrothorax following insertion of an external jugular vein catheter necessitating immediate drainage via a pigtail catheter insertion and mechanical ventilation. | | | | Case Report | A 15 days old female child, born vaginally at term gestation with birth weight of 2.3 kg presented with bilious vomiting. Urgent laprotomy showed localized volvulus of terminal ileum around a congenital band. The involved 15 cms of the distal ileum was gangrenous and had a large perforation at anti-mesenteric site. It was managed with resection of the gangrenous bowel with ileostomy and mucus fistula. The baby remained well postoperatively and was discharged home after 4 days on full feeds. The baby thrived well on ileostomy and was readmitted for stoma closure after 6 weeks from the day of first surgery. On the day of ileocolic anastomosis right external jugular vein was cannulated in operation theatre with 22 –gauge, 2.5 cms long intravenous (IV) cannula. There was good back flow of blood and this cannula worked smoothly during the surgery. Post operatively this IV line was used for intravenous fluids and antibiotics. Postoperatively up to 48 hrs the baby remained hemodynamically stable on room air with a normal general physical examination and X-ray chest. On 3rd post operative day there was sudden deterioration in general condition with severe respiratory distress and marked desaturation. Clinical examination revealed a respiratory rate of 70/minute and absent air entry on the right hemithorax with negative transillumination test. Soon the patient started to develop gasping breathing, severe bradycardia and cyanosis with oxygen saturation dropping to as low as 30% necessitating immediate tracheal intubation with positive pressure ventilation by bag and mask and cardiac massage .The patient was immediately shifted to intensive care unit (ICU) with mechanical ventilation support. Bedside anteroposterior chest radiograph was performed as shown in figure 1, which revealed complete opacification of the right lung and mediastinal shift to the left suggestive of massive right side pleural effusion. It was immediately confirmed by bedside ultrasound of chest followed immediately by insertion of a 28- French pigtail catheter under ultrasonographic guidance by interventional radiologist. A total of 80 cc of clear fluid was obtained from the chest drain, which was compatible with the fluid the patient received through the intravenous catheter. The external jugular vein cannula was removed and two peripheral lines were inserted for intravenous fluids and medications. The patient's condition improved with marked relief of the respiratory distress and improvement of the oxygenation. Follow-up chest X ray (figure 2) done after 12 hours showed good expansion of right lung with no re-accumulation of fluid hence the baby was extubated and chest drain was removed the next day. After this the baby recovered well and oral feeds were established on 5th post operative day. The baby was discharged home in good general condition and chest X-ray done at one month follow up visit was normal.
Fig 1: Chest X-ray showing complete opacification of the right hemithorax with mediastinal shift to the left suggestive of massive right side pleural effusion.
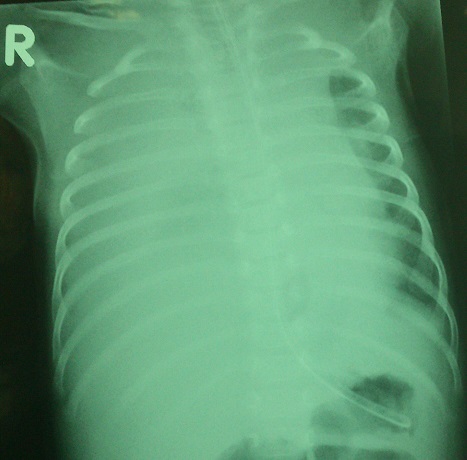
Fig 2: The pleural effusion on right side resolved completely after drainage by a pigtail catheter
 | | | | Discussion | | External jugular vein has an impressive safety profile due to its superficial position and distance from vital structures, thus decreasing the risk of major complications which are commonly associated with central venous lines. (5) However, as with all other invasive procedures, external jugular venous catheter placement is not free of complications. (6) In our case extensive extravasations of fluid in the right pleura happened 2 days after right external jugular vein cannulation resulting into massive right sided hydrothorax with mediastinal shift to opposite side requiring immediate drainage and mechanical ventilation. To the best of our knowledge this is a very rare delayed complication of right external jugular vein cannulation possibly related to movement of the child leading to pleural puncturing. This complication has been previously described on one occasion by Bitar et al in a neonate however the effusion in that case was bilateral and presented within hours of placement of catheter. (7) In our patient the clear colour of the fluid retrieved from the intercostal catheter, identical to that retrieved from the jugular catheter and the stoppage of effusion after removal of the cannula, all confirmed the intrapleural pouring of fluids administered through the cannula. Fortunately, the pleural effusion resolved completely without any sequelae following the detection of this complication and early management. The clinical signs of sudden respiratory distress with reduced breath sounds and displaced cardiac apex in a patient with external jugular vein should alert the clinician to the possibility of catheter tip misplacement leading to air or fluid collection into the pleura. | | | | Conclusion | | External jugular vein catheterization is a very useful and relatively safe procedure but complications do occur. Therefore, it is important to be mindful of complications that can arise. Moreover, one should be conscious of the possibility of movement of the end of the catheter due to the movement or changes in the patient's position which can occur also at a later stage. When complications do arise, being aware that the cause could be related to the catheter can reduce the delay in making a proper diagnosis. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Hoffmann W, Weidmann B, Jansen W, Tauchert M. Infusion hydrothorax as a sequel of malposition of an internal jugular vein catheter. Med Klin 1988;83:496–498.
- Meoni MS, Paoletti F. A complication of central venous cathe- terization: penetration into the mediastinum. Minerva Anestesiol 1988;54:63–66. [PubMed]
- Galofre J, Agusti C, Montserrat JM. Horner syndrome originating from catheterization of the internal jugular vein. Rev Clin Esp 1988;182:396–397. [PubMed]
- Van Haeften TW, van Pampus EC, Boot H, Strack van Schijndel RJ, Thijs LG. Cardiac tamponade from misplaced central venous line in pericardiophrenic vein. Arch Intern Med 1988;148:1649–1650. [CrossRef] [PubMed]
- Pettit J. External jugular cannulation in infants and children. J Infusion Nursing. 2009;32: 93-97. [CrossRef] [PubMed]
- Gajre G, Ali SD. Mediastinal tamponade following external jugular vein cannulation. Indian Pediatr. 2001; 38: 1177-1180. [PubMed]
- Bitar FF, Obeid M, Dabbous I, Hayek P, Akel S, Mroueh S. Acute respiratory distress associated with external jugular vein catheterization in the newborn. Pediatr. Pulmonol. 2003; 36: 549–550. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2014.30
|
| Cite this article as: | | Jangid M K, Yadav S K. Rare Case of Massive Hydrothorax Following External Jugular Vein Cannulation. Pediatr Oncall J. 2014;11: 46-47. doi: 10.7199/ped.oncall.2014.30 |
|