S.S. Kashyape, R.S. Kashyape, Pawan Kashyape.
Shree Medical Research Centre, Kashyape Children Hospital, Nashik, Maharashtra, India.
ADDRESS FOR CORRESPONDENCE
Dr.S.S.Kashyape, President, Shree Medical Research Centre, Nashik.
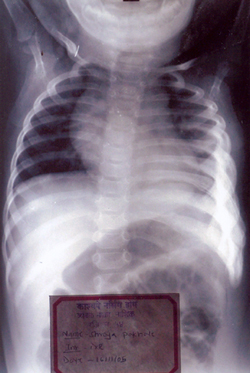
Email: dr_kashyape@rediffmail.com | Infantile cortical hyperostosis (Caffey's disease / ICH) is characterized by radiological evidence of cortical hyperostosis, soft tissue swelling and irritability. It may be familial or sporadic. A 7 months old girl born of term normal vaginal hospital delivery was brought with chief complaints of tender swelling over left side of chest in infraaxillary region extending from 3rd rib to 10th rib since 5 months and excessive irritability since 15 days. There was no history of trauma, fever, cough or breathlessness. There was no history of contact with tuberculosis or similar complaints in family. On examination the child was afebrile and vitals were stable. There was no pallor, icterus, clubbing, lymphadenopathy and edema. Systemic examination was normal. X-ray chest was done which showed pleural reaction with periosteal new bone formation of ribs.(Fig 1) Other investigations revealed normal hemogram and ESR. On the basis of clinical history and investigations the patient was diagnosed as a case of "ICH" and was started on oral ibuprofen 10 mg/kg/dose 8 hourly for 3 weeks. After 3 weeks irritability and swelling subsided, repeat x-ray chest was done which showed persistent pleural reaction with periosteal new bone formation of ribs.
Patients with Caffey's disease usually present around 9 weeks of age. The disease has been reported in utero. Several hypotheses have been proposed for the etiology of ICH. Since similar lesions have been described in infants who receive exogenous prostaglandins, one of the proposed mechanism is a disturbance of endogenous prostaglandin regulation. Some authors have tried prostaglandin inhibitors such as naproxen and indomethacin and Intravenous Gammaglobulin with some success.(1,2) Residual deformities may be seen very rarely upto adult life. Deformities and delayed muscular development may occur in the chronic stage. The severity of the disease may range from the barely perceptile to widespread involvement. Males and females are equally affected. The commonest site of bone involvement described in literature is the mandible followed by clavicles, ulna, scapula, tibia and ribs.(3,4) All bones of the body have been implicated except the phalanges, vertebral bodies and cuboidal bones. There may be asymmetrical involvement. Bone scan is more sensitive but less specific than CT scan or MRI for diagnosing ICH. There are no studies directly comparing these modalities. Most cases are sporadic, but autosomal dominant and autosomal recessive patterns have also been described.(5) The course of the illness is generally benign and recovers completely in many cases without treatment by 1 year.(6) | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Thometz JG,DiRaimando CA.A Case of recurrent caffey disease treated with naproxen.Clin Orthop 1996;323:304-309. [CrossRef]
- Couper RT,McPhee A,Morris L. Indomethacin treatment of infantile cortical hyperostosis in twins.J Pediar Child health 2001;37:305-308. [CrossRef]
- Mizrahi Mograbi L,de Id Calleja C. Cortical infantile hyperostosis.Report of a case and review of the literature.Bol Med Hosp Infant Mex 1977;34:315-324. [PubMed]
- Rethmeier JW.Infantile cortical hyperostosis.Two case reports.Radion Clin ( Basel ) 1976;45:251-257.
- Emmery L, Timmermans J,Christens J, Fryns. JP.Familial infantile cortical hyperostosis.EUR J Pediatr 1983;141:56-58. [CrossRef]
- Pohl A , Orha L , Dragoi AM.Infantile cortical hyperostosis.Rev Peditr Obstet Ginecol Pediatr 1989;38:369-373. [PubMed]
|
| Cite this article as: | | Kashyape S, Kashyape R, Kashyape P. Infantile Cortical Hyperostosis. Pediatr Oncall J. 2008;5: 84. |
|