Sravanthi K, Suneel Mundkur, Shrikiran Aroor, Sandeep Kumar, Harish Kashyap.
Department of Pediatrics, Kasturba Medical College, Manipal University, Manipal, India.
ADDRESS FOR CORRESPONDENCE
Dr Suneel C Mundkur, Department of Pediatrics, K M C Manipal, Karnataka, India.
Email: Suneel_cm@hotmail.com | | Keywords | | Yellow Oleander, Poisoning | | | The two common species Nerium oleander Linn (common, white, or pink oleander) and ThevetiaperuvianaJuss (yellow oleander) belong to the family Dogbaneapocynaceae. The yellow oleander (Thevetiaperuviana) is an ornamental tree that is common throughout the tropics and subtropics. (1) All parts of the plantincluding: stems, leaves, young shoots, flowers contain cardiac glycosides. (1)Ingestion of its seeds results in a clinical scenario similar to that of digoxin overdose. (2)Ingestionof an oleander seed is equal to that of swallowing 100 digoxin tablets in one container. (2)Severely poisoned patients may die in Direct current (DC)shock-resistant ventricular fibrillation. Many patients with moderate poisoning show PR interval prolongation and progression to atrioventricular (AV) dissociation. Accidental poisonings occur throughout the tropics, particularly in children. We report 2 children with yellow oleander poisoning.
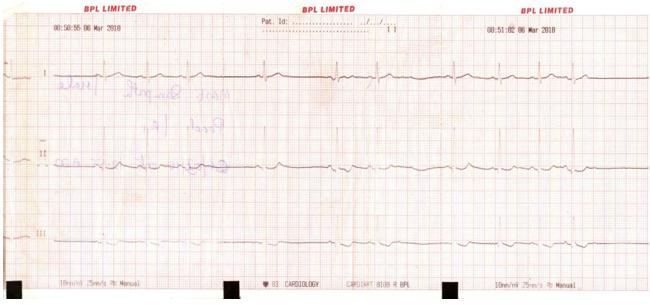
A 14 years oldboypresented with history of consumption of 1 oleander seedfollowed byvomiting, loose stools and giddiness. Examination revealed bradycardia with irregular rhythm. Stomach wash was given with activated charcoal. Electrocardiograph (ECG) showed sinus bradycardia with pauses (figure 1). Temporary pacemaker implantation was done. Pacemaker was removed at the end of 48hours as ECG showed normal pulse rhythm.Second child was a 15 years old girl who presented with 1 episode of vomiting following consumption of a crushed oleander seed. Examination revealed bradycardia with regular rhythm. ECG was suggestive of sinus bradycardia. She responded to atropine infusion. Repeat ECG done at the end of 48hours was normal.
Figure 1: ECG of patient (1) showing sinus bradycardia
There are very few studies on T.Peruviana poisoning especially in pediatric age group. (3)We report these cases to highlight the cardiac toxicity of Oleander poisoning even in small doses. The cardiac glycosides of Oleander produce more gastrointestinal effects than those in digoxin, and the symptoms range from nausea and vomiting to cramping and bloody diarrhea. (1) It causes burning and irritation of mucosal membranes. Confusion, dizziness, drowsiness, weakness, visual disturbances are neurological manifestations of toxicity.(3)Most serious side effects of Oleander poisoning are cardiac rhythm disturbances including ventricular dysrhythmias, tachyarrythmias, bradycardia, and heart block. ECG reveals prolonged PR interval, a decreased QRS-T interval, and T wave flattening/inversion. (3) Cardiac manifestations are due to vagotonia and direct cardiac glycoside toxicity. (3) Investigations include electrolytes and ECG. (4) Treatment consists of administration of a single dose ofactivated charcoal, treatment of hypotension or bradycardia with small bolus doses of atropine(0.3–0.6 mg) intravenously or as infusion (0.6 mg/hour) to maintain the normal heart rate, treatment ofco-existent hypokalemia and hypomagnesaemia. (2)AV node and/or severe sinus node block, ventricular tachycardia and serum potassium > 5.5 are indications for anti-digoxin Fab (400 mg over 20 min followed by 400–800 mg over 4–8 hours by infusion)if available. The best regimen is currently unclear. (1)Severe bradycardia due to AV block may require with temporary pacing.In the absence of anti-digoxin Fab, ventricular fibrillationis treated with low energy DC cardioversion. (1) | | | | Compliance with Ethical Standards | | Funding | | None | | | | Conflict of Interest | | None | | |
- Bandara V, Weinstein SA, White J, Eddleston M.A review of the natural history, toxinology, diagnosis and clinical management of Nerium oleander and Thevetiaperuviana poisoning. Toxicon. 2010;56:273-281 [CrossRef] [PubMed]
- Eddleston M, Ariaratnam CA, Sjöström L, Jayalath S, Rajakanthan K, Rajapakse S, et al. Acute yellow oleander (Thevetiaperuviana) poisoning: cardiac arrhythmias, electrolytedisturbances, and serum cardiac glycoside concentrations on presentation to hospital.Heart 2000;83:301–306 [CrossRef] [PubMed]
- Khan I, Kant C, Sanwaria A, Meena L.Acute Cardiac Toxicity of Nerium Oleander/Indicum Poisoning (Kaner) Poisoning. Heart Views. 2010;11:115-116. [CrossRef] [PubMed]
- Eddleston M, Warrell DA.Management of Yellow Oleander Poisoning. QJM. 1999;92:483-485. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2014.65
|
| Cite this article as: | | K S, Mundkur S, Aroor S, Kumar S, Kashyap H. Yellow Oleander Poisoning in Children- A Report of Two Cases. Pediatr Oncall J. 2014;11: 117-118. doi: 10.7199/ped.oncall.2014.65 |
|