V Poovazhagi1, Jegatheesh R1, Ganesa Pandian1, Singaravelu M1, Kavitha R2, Srinivasan A3.
1Department of Pediatrics, Raja Mirasdar hospital,
2Department of ENT, Thanjavur Medical College, Thanjavur, Tamil Nadu, India,
3Department of Radiology, Thanjavur Medical College, Thanjavur, Tamil Nadu, India.
ADDRESS FOR CORRESPONDENCE
Poovazhagi V, 8/11 Manjolai street, Kalaiamagal Nagar, Ekkaduthangal, Chennai 600032, India. Email: poomuthu@yahoo.com | | Keywords | | Acute Mastoiditis, Epidural abscess, extracranial complications | | | A 10 years old girl presented with fever, headache, vomiting, neck pain, ear discharge and lethargy for 5 days. She had been treated for acute otitis media a year ago. On examination, she was febrile, sick looking, had pus discharge from the right ear with tenderness and fullness over the mastoid region. Neurological examination revealed lethargy, normal deep tendon reflexes, bilateral extensor plantars and neck stiffness. Other systemic examination was normal. Incision and drainage of mastoid revealed pus which was sent for culture and hemogram revealed leucocytosis. In the next 24 hours, she developed bilateral abducent nerve palsy with intense headache. MRI brain and ears revealed right acute mastoiditis with an epidural abscess in the right anterosuperior aspect of the posterior fossa with compression of the right cerebellar hemisphere with right transverse sinus thrombosis extending onto the right internal jugular vein. CT temporal bone revealed erosion and opacification of the right mastoid cells with erosion of the lateral surface with pus collection in the subcutaneous plane posterior to the ear lobe and erosion of the right middle ear ossicles (Fig 1). She was treated with vancomycin, ceftriaxone, metronidazole, steroids, antiedema measures and antipyretics. Lumbar puncture revealed clear cerebrospinal fluid (CSF) with proteins 18mg/dl and sugar was 70mg/dl. Microscopy showed no cells and culture was sterile. She underwent burr hole incision and drainage of the abscess twice. Gram stain revealed gram positive cocci but the culture did not reveal any growth. Antibiotics were given for 21 days and then child underwent mastoidectomy. Child recovered uneventfully and was discharged after hospitalization for 8 weeks.
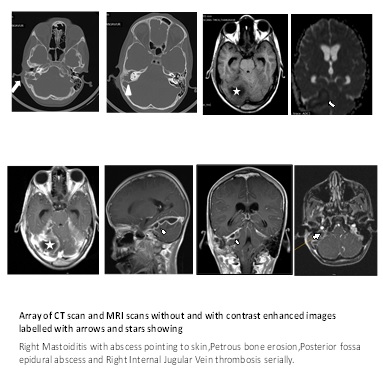
Figure 1: CT and MRI scans showing right mastoiditis with abscess pointing to skin, petrous bone erosion, posterior fossa epidural abscess and right internal jugular vein thrombosis (marked serially)
Prior to the antibiotic era nearly 25-50% of acute otitis media had complications as mastoiditis, subperiosteal abscess and sinus thrombophlebitis, 2-6 % of them had suppurative intra cranial complications and nearly 75% died. (1) Despite the advent of antibiotics, mastoiditis and the suppurative complications still cause problem probably due to the improper antibiotic exposure (2) or the antibiotic exposure masks the symptoms of mastoiditis. (3) Mastoiditis may result in serious intracranial complications. Abscess may form in the posterior or the middle cranial fossa. Sigmoid sinus thrombophlebitis may extend into the internal jugular vein. Thrombophlebitis can occur via the draining veins communicating with the dura leading on to subdural empyema. Intracranial complications are encountered in nearly 6.5% of mastoiditis. (4) Epidural abscess is the commonest intracranial complication. (2) Other complications include facial nerve palsy (2) subperiosteal abscess (2), bezold’s abscess (5), hearing loss (6), labyrinthitis (6) and petrositis (6).
Combined antibiotic therapy and mastoidectomy has decreased the mortality in mastoiditis. Surgical intervention, drainage of abscess and antibiotic therapy is the line of management. (7) Vigilant post operative care is mandatory as reaccumulation of the subperiosteal abscess is known to occur. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Zanetti D, Nassif N. Indications for surgery in acute mastoiditis and their complications in children. Int J Pediatr Otorhinolaryngol 2006; 70: 1175-1182. [CrossRef]
- Kuczkowski J, Narozny W, Stankiewicz C, Brzozowski W, Dubaniewicz-Wybieralska M, Plichta L. Epidural abscess as a complication of acute mastoiditis in a 7-year-old child. Otolaryngol Pol. 2010; 64: 320-323 [CrossRef]
- Cohen-Kerem R, Uri N, Rennert H, Peled N, Greenberg E, Efrat M. Acute mastoiditis in children: is surgical treatment necessary? J Laryngol Otol. 1999; 113: 1081–1085. [CrossRef]
- Psarommatis IM, Voudouris C, Douros K, Giannakopoulos P, Bairamis T, Carabinos C. Algorithmic management of pediatric acute mastoiditis. Int J Pediatr Otorhinolaryngol. 2012;76:791-796. [CrossRef]
- Marioni G, de Fillipis C, Tregnaghi A. Bezold's abscess in children : a case report and review of the literature. Int J Pediatr Otorhinolaryngol. 2001; 61: 173-177. [CrossRef]
- Goldstein N, Casselbrant M, Bluestone C. Intratemporal complications of acute otitis media in infants and children. Otolaryngol. Head Neck Surg. 1998; 119: 444-454. [CrossRef]
- Seung No H, Young Ho K, Chong Sun K. A Case of Acute Mastoiditis Complicated with Epidural Abscess. Korean J Otorhinolaryngol-Head Neck Surg. 2013; 56: 516-521. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2015.4
|
| Cite this article as: | | Poovazhagi V, R J, Pandian G, M S, R K, A S. Complications of Acute Mastoiditis in a Child in this Era of Antibiotics. Pediatr Oncall J. 2015;12: 24-25. doi: 10.7199/ped.oncall.2015.4 |
|