João Sousa Marques, Inês Silva Costa, Ana Gisela Oliveira, Clara Gomes
Department of Pediatrics, Centro Hospitalar Tondela-Viseu, Viseu, Portugal
Address for Correspondence: João Sousa Marques, Rua Monte Cativo, nº 247, 4050-401, Porto, Portugal.
Email: jnsmarques93@gmail.com
|
Question :A 16-year-old healthy male adolescent presented in the Emergency Department with right pleuritic chest pain extending to neck, that started suddenly seven hours before admission, without previous history of trauma or other symptoms.
Physical examination was unremarkable, except for the presence of localised tenderness inflicted by palpation of the 2 nd and 3 rd right intercostal spaces and ipsilateral sternocleidomastoid muscle. Chest radiography revealed a right linear lucency outlining mediastinal contours, of inconclusive nature. (Figure 1) The resting electrocardiogram was normal for age. On the first day of admission, a swelling and subcutaneous emphysema were noted on the right sternal border between 2 nd/3 rd intercostal spaces. The chest ultrasound showed the presence of air bubbles in the intermuscular spaces. The Computed Tomography (CT) Scan of chest and neck confirmed the presence of air distributed bilaterally in the mediastinum, mainly on the right side and extending to the neck and dissecting the anatomical planes of the upper mediastinum. (Figure 2)
Figure 1. Posteroanterior plain chest radiograph showing right linear lucency outlining mediastinal contours (arrow). 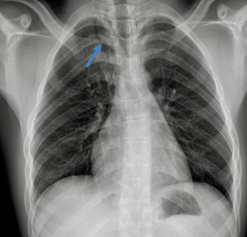 Figure 2.
Figure 2. Patient chest computed tomography scan shows presence of interstitial air distributed bilaterally in the mediastinum, mainly on the right side and extending to the neck, and dissecting the anatomical planes of the upper mediastinum (arrows). 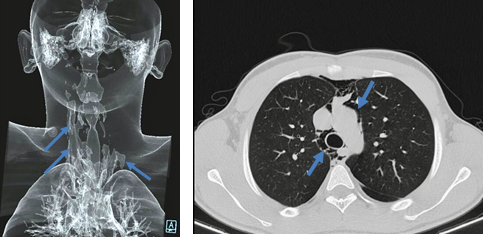 What is the diagnosis?
|
Discussion :
In this context, oxygen therapy was started with a reservoir mask at 15 L/min for five days, with clinical and imaging improvement and he was discharged six days after admission. At 6-month follow-up, the patient remained symptom-free and without evidence of recurrence.
Spontaneous pneumomediastinum (SPM) is a rare entity in paediatric age, defined by the presence of free air in the mediastinum, without traumatic cause. It´s usually associated with asthma, mainly affecting thin adolescents. 1,2
SPM is detected in young people often without apparent precipitating factors or diseases. Previous studies have been reported that the cause is related to an increase in alveolar pressure. 3 According to the Macklin effect, SPM is a result of rupture along the alveolar tree, which leads to an abrupt increase in the intra-alveolar pressure. Released alveolar air centripetally dissects through the pulmonary interstitium along the bronchovascular sheaths toward the pulmonary hila, into the mediastinum. A Macklin effect seen on CT scan may help to differentiate respiratory causes from other etiologies of pneumomediastinum. 4
In this case report the diagnosis of SPM was assumed after the CT scan of chest and neck confirmed the presence of air distributed bilaterally in the mediastinum extending to the neck and dissecting the anatomical planes of the upper mediastinum, presumably as a consequence of the alveolar rupture and further dissection along the axial interstitium (Macklin effect). 4
Uncomplicated SPM is usually an indolent condition that resolves in a few days and recurs rarely. Valsalva manoeuvres and activities predisposing to barotraumas must be discouraged. 2,5
It is important to bear in mind this rare condition that should be considered in the differential diagnosis of acute chest pain. | References : | - Noorbakhsh KA, Williams AE, Langham JJ, et al. Management and Outcomes of Spontaneous pneumomediastinum in children. Pediatric Emergency Care. 2021 Dec 1; 37(12):e1051-6. DOI: 10.1097/PEC.0000000000001895.
- Macia I, Moya J, Ramos R, et al. Spontaneous pneumomediastinum: 41 cases. European Journal of Cardio-Thoracic Surgery. 2007 Jun 1; 31 (6):1110-4. DOI: 10.1016/j.ejcts.2007.03.008.
- Kobayakawa A, Hiraiwa H, Ishizuka S, et al. Spontaneous Pneumomediastinum in an Adolescent Soccer Player. Journal of Sports Science & Medicine. 2021 Mar 1 ;20(1):52. DOI: 10.52082/jssm.2021.52.
- Murayama S, Gibo S. Spontaneous pneumomediastinum and Macklin effect: Overview and appearance on computed tomography. World J Radiol 2014; 6(11): 850-854. DOI: 10.4329/wjr.v6.i11.850.
- Fitzwater JW, Silva NN, Knight CG, et al. Management of spontaneous pneumomediastinum in children. Journal of Pediatric Surgery. 2015 Jun 1;50(6):983-6. DOI: 10.1016/j.jpedsurg.2015.03.024.
|
|
| Correct Answers : |  100% 100% |
Last Shown : Nov 2025
|