Arrhythmia
Sachin G Damke, Tushar Jagzape, Siddharth Kulkarni, Bhavana Lakhkar
Department of Pediatrics, JNMC, AVBR Hospital, Sawangi Meghe, Wardha, Maharashtra, India
Address for Correspondence: Sachin G Damke, Assistant Professor, Department of Pediatrics, JNMC, AVBR Hospital, Sawangi {Meghe}, Wardha, Maharashtra 442004.
Email: buntydamke@yahoo.com
Clinical Problem :
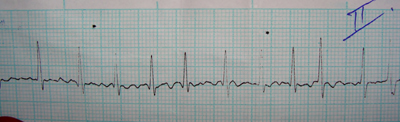
A 12 years old child, a diagnosed case of Rheumatic heart disease with mitral regurgitation with mitral stenosis with mild pulmonary hypertension presented to us with increasing breathlessness since 8 days. There was no history of fever. On examination, he was afebrile with a irregularly irregular heart rate of around 160 per minute, respiratory rate of 44 per minute, blood pressure of 92-60 mm of mercury, cardiomegaly and hepatomegaly. Chest X-ray showed cardiomegaly. Pre treatment ECG Lead II {Figure 1} is depicted below. 2D Echo showed grossly dilated left atrium and left ventricle, severe mitral regurgitation, mild mitral stenosis, mild pulmonary hypertension.
Figure 1: Lead II ECG
|
What is the diagnosis_?
Discussion :
Atrial fibrillation {AF}. AF is less common in children and rare in infants. The atrial excitation is chaotic and more rapid {300–700 beats per min} and produces an irregularly irregular ventricular response and pulse. AF is most often the result of a chronically stretched atrial myocardium. It occurs most frequently in older children with rheumatic mitral valve disease. It is also seen rarely as a complication of intra-atrial surgery, in patients with left atrial enlargement secondary to left AV valve insufficiency, in conditions producing atrial flutter, and in patients with WPW syndrome. Thyrotoxicosis, pulmonary emboli, and pericarditis should be suspected in a previously normal older child or adolescent with atrial fibrillation. Atrial fibrillation may be familial. The best initial treatment is digitalization, which restores the ventricular rate to normal, although the atrial fibrillation usually persists. Digoxin is not given if WPW syndrome is present. Normal sinus rhythm may then be restored with a type I agent {quinidine or procainamide}, with amiodarone, or by DC cardioversion. Patients with chronic atrial fibrillation are at risk for the development of thromboemboli and stroke and should undergo anticoagulation with warfarin. Patients being treated by elective cardioversion should also undergo anticoagulation.
Last Updated: July 2011 Vol 8 Issue 7 Art No. 46
| Correct Answers : |  100% 100% |
|
|
|
|
|
|