Successful Recovery from HHV-6 Encephalitis in an Immunocompetent Child
Vaidehi Mehta1, Suhani Jain2, Meenakshi Dey1, Ira Shah1
1Department of Pediatric Infectious Diseases, B J Wadia Hospital for Children, Mumbai, India, 2Grant Government Medical College, Sir JJ Group of Hospitals, Mumbai, India
Address for Correspondence: Suhani Jain, Flat number 402, Ramdeo Arise, Behind Hotel Airport Centre Pt, Wardha Road, Nagpur-440025.
Email: suhani2208@gmail.com
Keywords: HHV6 encephalitis, Ganciclovir, Prognosis
Clinical Problem :
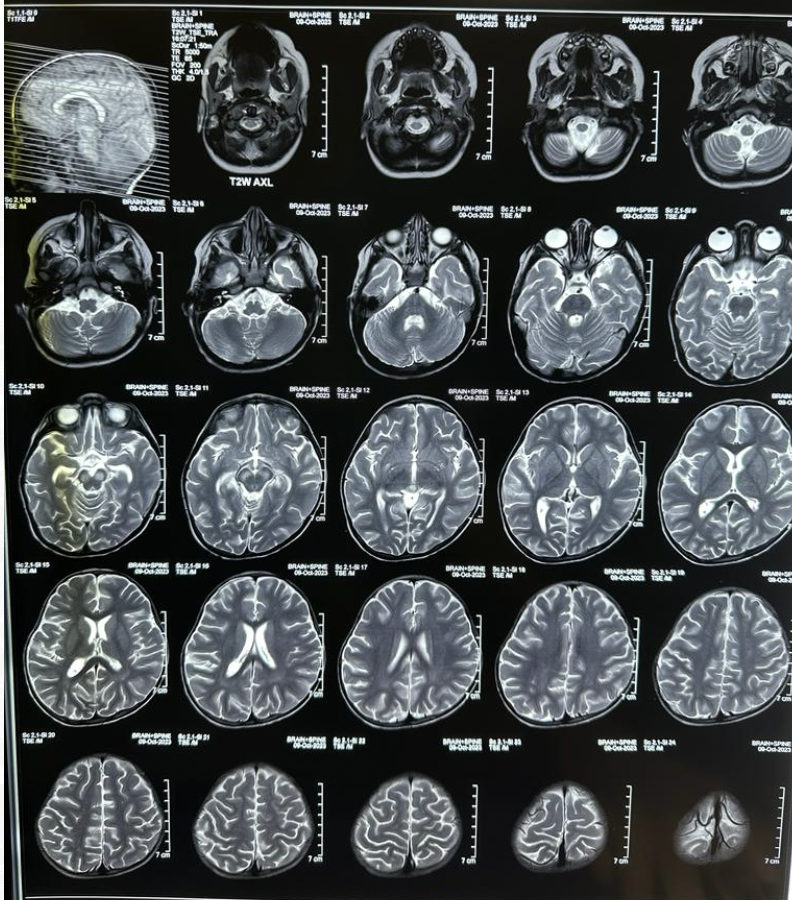
A 2-year-old female child presented with a 10 day history of persistent fever and an episode of paroxysmal event on the 1st day of illness. Her family history was unremarkable and vaccinations were up-to-date. She had no history of Tuberculosis (TB) contact. She was hospitalised for the above complaints with altered sensorium at a private hospital and she was given Amikacin for 5 days, piperacillin-tazobactam for 3 days, Ceftriaxone for 2 days and Artesunate for 5 days. On day 5th of hospitalization, the child further deteriorated as she developed aphasia and neck stiffness and was transferred to another hospital for further management. Cerebrospinal Fluid (CSF) analysis was done which indicated elevated protein (60 mg/dl), normal sugars (56 mg/dl) and cell count of 40 cells/cumm with neutrophils 12 cells/cumm and lymphocytes 28 cells/cumm. Multiplex meningitis PCR panel was positive for HHV-6. Additionally, blood culture grew Acinetobacter baumanii. MRI was done which was suggestive of bilateral frontoparietal and temporal cortical sulcal spaces suggestive of encephalitis with meningitis (Figure 1). Child received Meropenem for 5 days, Vancomycin for 5 days, Acyclovir at 10 mg/kg/dose 8 hourly for 5 days and Methylprednisolone (30 mg/kg/day) for 3 days. She was subsequently referred to our institute for further management. On presentation to us, she was afebrile but there was neck stiffness. Glasglow coma scale (GCS) was 12/15. Her heart rate was 124/min, respiratory rate was 28/min and blood pressure was 102/64 mm of Hg (90th -95th centile). Weight was 9.8 kg (3rd -15th centile as per World Health Organization (WHO) charts) and height was 90 cm (75th – 90th centile as per WHO charts). Other general examination findings were normal. Central nervous system (CNS) examination revealed meningeal irritation with brisk deep tendon reflexes. There was hypertonia. There was no focal neurological deficit. Other systemic examination was unremarkable. Complete Blood Count (CBC) revealed Hemoglobin (Hb) - 9.7 g/dL, platelet count was 819 x 103/µL, total leukocyte count (TLC) was 5190 cells/µL (neutrophils – 35% and Lymphocytes – 45%). C- Reactive Protein (CRP) was 0.7 mg/dl on admission. The human immunodeficiency virus (HIV) screening by ELISA was negative. Antibiotics were changed to intravenous Levofloxacin and amikacin. Injectable Ganciclovir (5 mg/kg 12 hourly) was also started in view of HHV-6 virus for 21 days. Patient also received Intravenous Immunoglobulin at 2 gram/kg and Methylprednisolone was continued and given for total for 5 days. A repeat MRI brain was done which showed mild brain volume loss. Previously seen tiny foci of restricted diffusion in bilateral cerebral hemispheres were not seen in this scan. And both substansia nigra also showed T2 /Flair hyperintense and does not show restricted diffusion (Figure 2). Patient also had another episode of paroxysmal event and was started on levitercetam and Levodopa for the same. Post 25 days of hospital stay, the child show T2 /Flair hyperintense and does not show restricted diffusion recovered with no signs of neurological deficit and speech returned to normal. Currently she is on tapering doses of Levodopa and leviteracetam has been continued.
Figure 1. MRI suggestive of bilateral frontoparietal and temporal cortical sulcal spaces suggestive of encephalitis with meningitis.

Figure 2. Previously seen tiny foci of restricted diffusion in bilateral cerebral hemispheres not seen. Both substantia nigra also show T2/Flair hyperintense and does not show restricted diffusion.
|
Should HHV-6 isolated in the CSF be treated with antivirals and which antivirals?
Discussion :
HHV-6 is very rare in immunocompetent children. Primary infection usually occurs in first two years of life which was seen in our patient. Having neurotropic properties it can manifest as irritability before rash in patients. The virus can directly affect the central nervous system (CNS) by causing inflammation of neurons and increasing the excitability of neurons causing febrile seizure/convulsion. Convulsion also cause inflammation of neurons hence making it a viscous cycle. 1 In our patient child had one episode of paroxysmal event on the 1st day of illness itself without any prior rash and had another episode of convulsion at our institute after which child was started on levitercetam for control of convulsion.
The disease is usually self limiting in immunocompetent children and does not require any treatment. But since this child had meningoencephalitis on MRI Brain and multiplex meningitis PCR on CSF detected HHV-6, treatment for this child was warranted. Another relevant differential in the child’s history was the growth of A.baumanii in the blood sample. However, since A.baumanii meningitis typically correlates with foreign material placement and presents differently in CSF and MRI results, it could be eliminated as the likely cause of the patient's symptoms 2 therefore, allowing the confirmation of HHV-6 encephalitis diagnosis in our patient
The use of Methylprednisolone and IVIG helped in immunomodulation and reduce the neuroinflammation caused by the virus leading to decreased inflammation induced damage to the nervous system. 3
Antivirals like ganciclovir, Foscarnet and Cidofovir are used for treating HHV-6 induced encephalitis. Ganciclovir and Foscarnet is preferred over Cidofovir as it is nephrotoxic. 4 We gave injectable Ganciclovir (5 mg/kg 12 hourly) for 21 days and child recovered without any focal neurological deficit and aphasia was also completely resolved.
To conclude in pediatric populations whenever meningoencephalitis is present viral etiology should also be considered. Atypical presentations should also be kept in mind for a elaborative approach and prompt adjustment in treatment with supportive management is necessary for a positive outcome. | References : | - Komaroff, A.L.; Pellett, P.E.; Jacobson, S. Human Herpesviruses 6A and 6B in Brain Diseases: Association versus Causation. Clin. Microbiol. Rev.2020, 34, 2-36.
- Xiao J, Zhang C, Ye S. Acinetobacter baumannii meningitis in children: a case series and literature review. Infection. 2019 Aug 1;47(4):643-9.
- Prasad, R., & Kapoor, R. (2018). Methylprednisolone in acute disseminated encephalomyelitis: A systematic review and meta-analysis. Neurology India, 66(5), 1261-1267.
- Agut Henri, Bonnafous Pascale, Gautheret-Dejean Agnès. Laboratory and Clinical Aspects of Human Herpesvirus 6 Infections. Clinical Microbiology Reviews. 2015 Mar 11;28(2):313-35.
|
| Correct Answers : |  100% 100% |
|
|
|
|
|
|