Shravan Kanaparthi, Suneel C Mundkur, Kalyan Chakravarthy Konda, Shrikiran Aroor, Ujjwala Mantha.
Department of Paediatrics, Kasturba Medical College, Manipal, Manipal University, Karnataka, India.
ADDRESS FOR CORRESPONDENCE
Dr. Kalyan Chakravarthy Konda, Address: Flat No 206, Mandavi Sapphire, Perampalli road, Manipal, Karnataka, India- 576104.
Email: k.kalyan.22189@gmail.com | | Abstract | | Melioidosis is an infectious disease caused by a gram-negative bacillus, Burkholderia pseudomallei. It is known to be endemic in Southeast Asia and Northern Australia. There is a recent surge in cases from coastal India. We hereby report four episodes of Melioidosis in 3 children with one child having a recurrent episode. One child was male and two were female, with all the children aged more than ten years (range 10-14years). Fever was the most common symptom followed by abdominal and bone pain in 50% of episodes. Immunocompromised state (post-splenectomy status and steroid therapy) as a predisposing factor was present in 2 children. One child presented with septicemia and succumbed within 72 hours of admission. ceftazidime/Meropenem and cotrimoxazole were used in intensive and eradication phase respectively. A comprehensive knowledge and high index of suspicion are required to diagnose Melioidosis. Prolonged treatment course with appropriate antibiotics would help in minimizing the mortality and morbidity in children. | | | | Keywords | | Burkholderia, Melioidosis, abscess | | | | Introduction | Melioidosis is a zoonotic disease endemic in certain tropical regions of Southeast Asia and Northern Australia. Sporadic cases have been reported from the African and the American continents. It is caused by gram-negative bacillus Burkholderia pseudomallei. (1) B. pseudomallei can evolve rapidly during an acute infection in the same host with significant genetic diversity. (2) The intracellular survival of B. pseudomallei facilitates the disease pathogenesis. (1) Children may present with life-threatening infection necessitating a comprehensive knowledge about the condition and intensive medical care. We report three children who presented with Melioidosis to our institute.
Case 1: A 10 years old boy, suffering from beta-thalassemia major and on regular blood transfusion since infancy presented with fever and swollen, painful left knee joint for 15 days in May 2014. He had undergone splenectomy one year ago and was on daily oral penicillin prophylaxis. Examination revealed left knee joint effusion with hepatomegaly. X-ray of the knee joint showed lytic lesion in lateral condyle of the femur (Fig 1). Arthrotomy and drainage of pus was done. Pus culture grew B. pseudomallei. Blood culture was sterile. Ultrasound (USG) abdomen showed mild hepatomegaly without any evidence of abscess. He received intravenous (IV) ceftazidime for 14 days followed by oral cotrimoxazole (TMP-SMX) for three months following which he improved with resolution of osteomyelitis. He presented again two years later, in August 2016, with fever and abdominal pain for 3 weeks. Examination revealed tender hepatomegaly (span 16cm). There was no bone or joint involvement. USG abdomen and Contrast enhanced Computerized Tomography (CECT) abdomen revealed liver abscess in segment V/VI measuring 4 x 5 x 6cm and a sub-capsular abscess measuring 6.7 x 2 x 8cm in right lobe of liver (Fig 2). Laparotomy and drainage of the abscess was done. Pus culture revealed B. pseudomallei. Blood culture was sterile. He received IV meropenem for two weeks followed by tmp-smx for 5 months. He was followed up for one year, remained asymptomatic and follow-up USG showed resolution of liver abscess.
Case 2: An 11 years old girl presented in November 2015 with recurrent episodes of fever and abdominal pain for one-month duration. Examination revealed hepatosplenomegaly. USG abdomen and CECT abdomen showed hepatic abscess measuring 3 x 3 x 2cm in segments VI/VII and tiny splenic abscess (Fig 3 and 4). Blood culture grew B. pseudomallei. She was treated with IV ceftazidime and meropenem for two weeks followed by oral tmp-smx for 3 months. She became afebrile by day 7 of illness with repeat USG after 3 months showing resolved abscess.
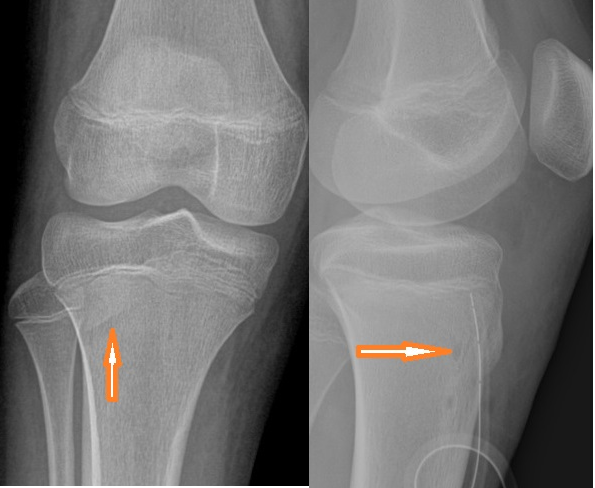
Case 3: A 14 years old girl, suffering from systemic lupus erythematosus (SLE) and on treatment with 1mg/kg/day of prednisolone on alternate day presented with fever and right knee joint pain for 10 days in August 2015. Examination revealed right knee joint effusion. X-ray showed minute lytic areas in proximal tibia (Fig 5). Decompression and debridement of right proximal tibia was done. On day two of the procedure, she developed worsening cough and respiratory distress. Her Blood culture grew B. pseudomallei and she was started on IV ceftazidime and meropenem due to her rapidly worsening condition. She was put on mechanical ventilation but succumbed to her illness on day 3 of admission.
Fig.1- X-ray showing osteomyelitis of lateral condyle of femur.

Fig 2- Computerized Tomography abdomen showing intrahepatic abscess.
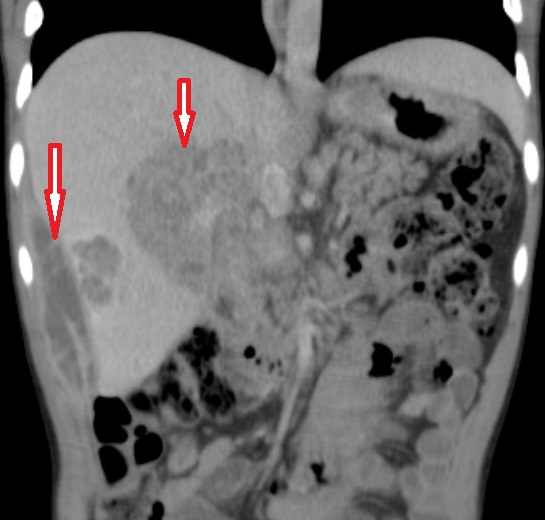
Fig.3 - Computerized Tomography abdomen showing intra-hepatic abscess.
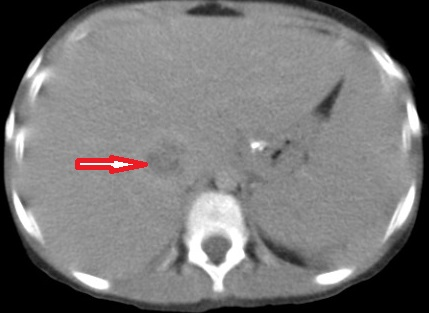
Fig.4 - Computerized Tomography abdomen showing tiny splenic abscess

Fig.5 - X-ray of tibia showing linear lucency (left image). X-ray of tibia showing lacunae and drain tube in-situ (right image).
| | | | Discussion | Melioidosis is predominantly seen during the rainy season and affects people who are frequently exposed to soil and water. In the present study, 2 out of 4 episodes, occurred during the rainy season. Routes of infection include percutaneous inoculation, inhalation and by ingestion. (3) Usually a disease affecting adults between 40-60 years of age, increased number of cases in children are being reported. (1) Children less than 15 years of age account for 5-8% of total melioidosis cases. Melioidosis is more common in children with predisposing factors like diabetes, thalassemia, chronic pulmonary and renal diseases, glucocorticoid therapy and in children with cancer. (1,3) In the present study, two children had predisposing factors, one had beta thalassemia major, and the other was on steroid treatment for SLE.
Clinical manifestations are highly variable ranging from fatal sepsis to chronic symptoms. Pneumonia, genitourinary tract infections skin infection, sepsis, septic arthritis, osteomyelitis, internal organ abscesses, suppurative parotitis and neurological involvement, may be seen. (3-5) Twenty-one percent of cases present with septic shock, with fatality ranging from 50-90% in cases of septicemia. Mortality rate is less in Australia (15%) whereas it is more in Thailand (around 49%). (4) Neonatal melioidosis presenting with pneumonia and meningitis in preterm and term children are reported in the literature. (6,7) Neuro-melioidosis consists most commonly of localized brain or spinal cord infections. Out of these, most are intra-axial (cerebellum, brainstem, and cerebrum) and few present with extra-axial lesions (skull osteomyelitis, epidural/subdural collection, scalp abscesses). (8) In the present study, fever was the most common symptom. Pain in abdomen and limb pain were seen in 2 out of 4 episodes. Abdominal abscesses and bone involvement were seen in 2 episodes (50%). Mortality was 33%, one child had septicemia and succumbed within 72 hours of admission.
Recurrence of Melioidosis is seen more commonly in the first year after the diagnosis. Relapse from a persistent focus is the most common cause of relapse (9.7% of cases), although few may be due to re-infection (3.4% of cases). Choice of antibiotic therapy, positive blood culture, and multifocal distribution are the most important determinants of risk of relapse. (9) Treatment duration for 12-16 weeks had a lesser risk of relapse when compared to treatment for eight weeks. (9,10) In the present report, one out of 3 children (33%) had recurrence two years after the initial infection. Retrospective analysis of risk factors for recurrence was done, and no other reason apart from being splenectomized was found.
Blood culture is the gold standard investigation for detecting B. pseudomallei (1) and is positive in 40% of cases. (9) Polymerase chain reaction (PCR) can be done on clinical samples. Serological tests are not recommended in endemic areas due to higher background positivity rate. (1) In our study, blood culture was positive in two children (2 out of 4 episodes) whereas pus cultures were positive in rest of the episodes.
Melioidosis needs a prolonged treatment for the complete cure of the disease. B. pseudomallei is resistant to aminoglycosides, penicillin, first and second generation cephalosporins, ampicillin and polymyxin. Treatment consists of an intensive phase lasting for 10-14 days followed by an eradication phase for 3-6 months. ceftazidime, meropenem or Imipenem are given parenterally in intensive phase and tmp-smx orally in eradication phase. (1,3,11) Amoxicillin-clavulanate and doxycycline can be used (12) however, are less efficacious than tmp-smx. Amoxicillin-clavulanate is recommended in pregnant women due to the adverse pregnancy outcomes associated with tmp-smx. (3) ceftazidime and meropenem was used in intensive phase treatment for two episodes, whereas ceftazidime and meropenem alone was used for one episode each. tmp-smx was used in eradication phase for all the episodes. Post-exposure prophylaxis with tmp-smx or amoxicillin-clavulanate for 21 days is recommended. (3) Blood culture should be repeated after one week of treatment. Worsening of clinical status after 48 hours of treatment and or positive blood culture after one week of treatment is considered as a ‘treatment failure'. Search for an underlying abscess and change of drugs from ceftazidime to meropenem is indicated. The addition of tmp-smx is advised if the child is already being treated with carbapenems. (3) Resistance to tmp-smx ranges from 2.5-13% in different parts of the world. (1) Resistance to ceftazidime was very minimal (0.6%) and to carbapenems was not found in a study in Thailand. (3,13)
| | | | Conclusion | | Melioidosis with its gradual global spread has posed as an important threat to the community. An increased clinical vigilance with good microbial work-up would help with improved, accurate and rapid diagnosis. Timely institution of appropriate antibiotics would help in reducing the mortality and continuation for recommended duration would help in reducing relapses and morbidity. | | | | Acknowledgement | | None | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Joost WW, Bart JC, Sharon JP. Melioidosis. N Engl J Med. 2012;367:1035–44. [CrossRef]
- Price EP, Hornstra HM, Limmathurotsakul D, Max TL, Sarovich DS, Vogler AJ, et al. Within-Host Evolution of Burkholderia pseudomallei in Four Cases of Acute Melioidosis. 2010;6(1).
- Lipsitz R, Garges S, Aurigemma R, Baccam P, Blaney DD, Cheng AC, et al. Workshop on Treatment of and Postexposure Prophylaxis for Burkholderia pseudomallei and B. mallei Infection. Emerging Infectious Diseases. 2010;18:2. [CrossRef]
- Currie BJ, Ward L, Cheng AC. The Epidemiology and Clinical Spectrum of Melioidosis : 540 Cases from the 20 Year Darwin Prospective Study. PLoS Negl Trop Dis. 2010;4(11):1–11. [CrossRef]
- Chirnajay M, Vandana KE, Pushpa Kini, Vinod B. Pediatric Melioidosis in Southern India. Indian Pediatr. 2015;52:711–2.
- Dinesh H, Nik Z, Chua MW, Ashraful H. Neonatal meningitis and septicaemia caused by Burkholderia pseudomallei. Ann Trop Paediatr. 1998;18:161–4. [CrossRef]
- Lumbiganon P, Pengsaa K, Puapermpoonsiri S, Puapairoj A. Neonatal melioidosis: a report of 5 cases. Pediatr Infect Dis J. 1988;7(9):634–6. [CrossRef]
- Fong SL, Shyanwong J, Tan AH, Low SC, Tan CT. Neurological melioidosis in East Malaysia : Case series and review of the literature. 2017;22(1):25–32.
- Limmathurotsakul D, Chaowagul W, Chierakul W, Stepniewska K, Maharjan B, Wuthiekanun V, et al. Risk factors for recurrent melioidosis in northeast Thailand. Clin Infect Dis. 2006;43(8):979–86. [CrossRef]
- Cheng AC, Currie BJ. Melioidosis: epidemiology, pathophysiology, and management. Clin Microbiol Rev. 2005;18(2):383–416. [CrossRef]
- Samuel M, Ti TY. Interventions for treating melioidosis. Cochrane database Syst Rev. 2002;(4):CD001263. [CrossRef]
- Schweizer HP. Mechanisms of antibiotic resistance in Burkholderia pseudomallei: implications for treatment of melioidosis. Future Microbiol. 2012;7(12):1389–99. [CrossRef]
- Wuthiekanun V, Amornchai P, Saiprom N, Chantratita N, Chierakul W, Koh GCKW, et al. Survey of Antimicrobial Resistance in Clinical Burkholderia pseudomallei Isolates over Two Decades in Northeast Thailand. Antimicrob Agents Chemother. 2011;55(11):5388–91. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2017.54
|
| Cite this article as: | | Kanaparthi S, Mundkur S C, Konda K C, Aroor S, Mantha U. Melioidosis in Children from Southern Coastal India. Pediatr Oncall J. 2017;14: 85-87. doi: 10.7199/ped.oncall.2017.54 |
|