A rare cause of chest pain in a teenager - an unlikely diagnosis
|
|
A rare cause of chest pain in a teenager - an unlikely diagnosis
05/02/2022
05/02/2022
https://www.pediatriconcall.com/Journal/images/journal_cover.jpg
Sofia Pimenta1, Carolina Fraga2, Manuel Ferreira1, Leonilde Machado1, Margarida Tavares3, Joaquim Cunha1.
1Pediatrics department, Centro Hospitalar Tâmega e Sousa, Penafiel, Portugal,
2Pediatrics department, Centro Materno Infantil do Norte, Centro Hospitalar Universitário do Porto, Porto, Portugal,
3Pediatric Infectious Diseases and Primary Immunodeficiencies Unit, Centro Hospitalar São João, Porto, Portugal.
ADDRESS FOR CORRESPONDENCE
Sofia Pimenta, Avenida do Hospital Padre Américo, Nº 210 Guilhufe, Penafiel - Centro Hospitalar Tâmega e Sousa
Email: sofiapimentaa@gmail.com
hydatidosis, echinococcus, chest pain
|
Clinical Problem
A 12-year-old female born in Syria presented to the emergency department with a history of fever and rhinorrhea for the last 2 weeks. She had been prescribed amoxicillin without improvement, and she began to complain of right chest pain. She showed no signs of respiratory distress, and pulmonary auscultation revealed decreased breath sounds over the right lung. Her past medical history, apart from an unmonitored pregnancy, was irrelevant. She had recently received her first immunizations because she was a war refugee, having lived in a refugee camp in Turkey for the last 5 years.
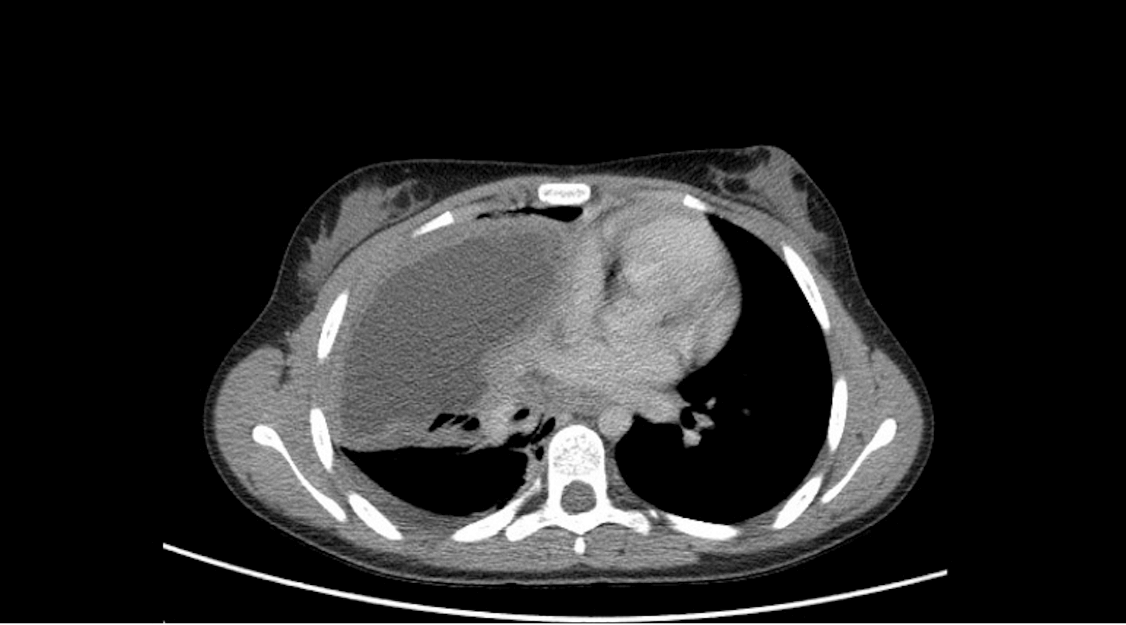
A chest x-ray was performed and revealed a large, oval, well-defined, and hypodense mass in the middle part of her right chest. Therefore a chest CT scan (Figure 1) revealed a lesion on the medium right lobe with regular contours, thin walls, and hypodense content, suggesting a probable congenital malformation, such as a bronchogenic cyst, or less likely, a hydatid cyst.
Figure 1. Chest CT revealed a lesion on the medium right lobe with regular contours, thin walls, and hypodense content.
|
| |
What is the diagnosis?
|
|
|
Discussion
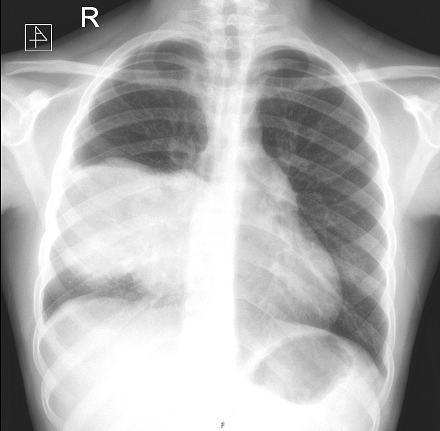
Lab results showed eosinophilia (1,490/uL) and increased erythrocyte sedimentation rate (30 mm/h). The patient was hospitalised and albendazole was started. Her serology for Echinococcus was positive. Eleven days later, her fever returned with a worsening cough. Chest x-ray (Figure 2) revealed signs of cyst rupture. A cyst excision and lobectomy were performed, and the presence of Echinococcus was confirmed in the cystic fluid. She completed 6 months of albendazole and had no recurrence after 3 years of follow-up.
Hydatidosis is a zoonotic disease with worldwide distribution, and humans are an accidental host.1 Definitive hosts, usually dogs, hold adult tapeworms in their small intestine which release numerous eggs through faeces to the environment. The eggs are ingested by intermediate host (domestic animals) or accidental hosts (humans, through contaminated water or vegetables) and from them hatch oncospheres, which migrate through blood and lymphatic system to visceral organs, primarily the liver. There, they form vesicles which in a few days maturate into fluid-filled cysts (hydatid cysts). Within these cysts, protoscolices develop and, if ingested by definitive host, they evaginate and develop into adult tapeworms, completing echinococcus life cycle.1 In humans, hydatic cysts are mostly caused by Ecchinococcus granulosus and Ecchinococcus multilocularis and have a highly variable growth rate.2
The diagnosis of a hydatid cyst on the lung (the second most common location) is often an incidental finding in an asymptomatic patient.1 Eosinophilia may be present in less than 15% of cases.2 Symptoms may develop from compression (cough, chest pain, dyspnoea) or due to cyst rupture, either with respiratory distress or anaphylaxis.1,2 Treatment may be conservative (either observational or pharmacological) for simple cysts, although surgical excision or percutaneous drainage may be necessary for complex or complicated cysts.3 A follow-up period of 3-5 years is recommended due to the risk of recurrence.3
This diagnosis should be considered in the presence of suggestive imaging results in order to begin treatment early and reduce the risk of complications.
Figure 2. Chest x-ray revealed a bilobed hypodense mass on the right chest, compatible with cyst rupture.
|
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
- Lupia T, Corcione S, Guerrera F, et al. Pulmonary Echinococcosis or Lung Hydatidosis: A Narrative Review. Surg Infect (Larchmt). 2021 Jun;22(5):485-495. doi: 10.1089/sur.2020.197. Epub 2020 Dec 9. PMID: 33297827. [CrossRef] [PubMed]
- Moro, PL. Clinical Manifestations and Diagnosis of Echinococcosis, In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on July 30, 2021.)
- Moro, PL. Treatment of Echinococcosis, In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on July 30, 2021.)
|
|
| |
Cite this article as:
Pimenta S, Fraga C, Ferreira M, Machado L, Tavares M, Cunha J. A rare cause of chest pain in a teenager - an unlikely diagnosis. Pediatr Oncall J. 2022;19: 107-108. doi: 10.7199/ped.oncall.2022.36
|