Abdul qadeer1, Khatidja Ally1, Hira Waseem1, Hina Rajani1, Ashar Masood Khan2.
1National institute of child health, Karachi, Pakistan,
2Dr Ziauddin University hospital, Karachi, Pakistan.
ADDRESS FOR CORRESPONDENCE
Ashar Masood Khan, SF2 Block 7 Seaview Apartments Dha Phase 5, Karachi - 75500, Pakistan.
Email: asharmasood65@gmail.com | | Keywords | | Filling defects, Multi-system inflammatory syndrome, COVID-19. | | | | Abstract | | SARS-Cov-2, commonly known as severe acute respiratory syndrome, is primarily asymptomatic or mild in severity in children, as documented by the COVID-19 spread.1 A unique problem during this worldwide outbreak has been the emergence of "multi-system inflammatory syndrome in children (MIS-C), a rare post-infectious hyper-inflammatory disorder associated with SARS-CoV-2". The patient can present with characteristics such as signs of congestive heart failure, pyrexia, hypotension, and inflammatory conditions. Additionally, this illness has features similar to toxic shock syndrome (TSS), macrophage activation syndrome (MAS), and Kawasaki disease (KD). The purpose of this report is outlining the presenting characteristics, suspected immunopathogenesis, treatment, and prognosis of MIS-C patients. | | | | Introduction | | The official term for the SARS-CoV2-caused illness is COVID-19 (Coronavirus disease of 2019). City of wuhan, china was supposidely the center of spread of the disease from were the first case emerged by the end of 2019 and soon after the pandemic started to pose a threat to the entire planet. It has affected around 49 million individuals and more than a million people have died from it, becoming a global health burden and leaving some rare but debilitating consequences on the health of affected individuals.2 There have been numerous reports in which patients suffering from COVID-19 have developed complications like thromboembolism, including coagulopathy in several organs such as the brain, lungs, spleen, legs and heart. Severe form of this diseases leads to complications like multi organ failure and significant fatality rates. According to available clinical data,“ Pulmonary embolism (PE) and deep vein thrombosis (DVT) are the most frequently observed thrombotic events in COVID-19”. Despite receiving anticoagulation prophylaxis, the probability of developing venous thromboembolism (VTE) is still significant among hospitalized patients.3 | | | | Case Report | Clinical Presentation:
A 7 year old male child was admitted at the National Institute of Child Health with a complaint of jaundice for 6 days. The child had a fever 10 days back which subsided after 4 days. After that, the parents noted yellowish discoloration of sclera. There was no history of melena, concentrated urine, abdominal distension, pain, vomiting, hematemesis, skin rash, itching, conjunctival hyperemia, or respiratory distress. The family drank tap water and had a poor hygienic lifestyle.
The child has an history of Ventricular septal defect (VSD), Atrial septal defect (ASD), Dextro-Transposition of the Great Arteries (d-TGA) and Severe Pulmonary Stenosis. Significant procedures like Blalock-Taussig (BT) Shunt and Glen shunt were done in 2018 and 2021 respectively.
On presentation, the child was thin and lean with an icterus. The child weighed 16 kg (25the centiles) with a heart rate of 88 beats/min and respiratory rate of 28/min. BP readings were <50the centile while clubbing was grading 3 positive.
On pericardium examination, S1 and S2 heart sounds were audible with holosystolic murmur at the left lower sternal border. On chest examination, 2 scar marks were seen extending from the sternal angle to the xiphoid space process and at the 6th intercostal space from the midclavicular line to the posterior axillary line.
On abdominal palpation, the liver was palpable 5 cm BRCM with a liver span of 16 cm, smooth surface, and regular margins. No splenomegaly was appreciated.
Investigation:
On lab investigation, CBC showed a total leukocyte count of 8900/cm with neutrophils at 60% and lymphocytes at 32%. Reticulocyte counts 3.70, increased total bilirubin of 10.7 with direct bilirubin of 5.3 and SGPT 86.
To investigate further the possible cause of hepatitis in this patient, a serological test for viral hepatitis and a test to evaluate possible autoimmune hepatitis were performed. The child showed a positive IgM for hepatitis A while the rest of the tests were negative. The ultrasound of the abdomen was done to look for liver echotexture, which was normal but, the heterogeneous pancreas was seen, however serum amylase and lipase were normal.
CT abdomen was done which showed hepatomegaly, edematous gallbladder with clinical pericholecystic fluid resulting in periportal tracking and few prominent para-aortic lymph nodes.
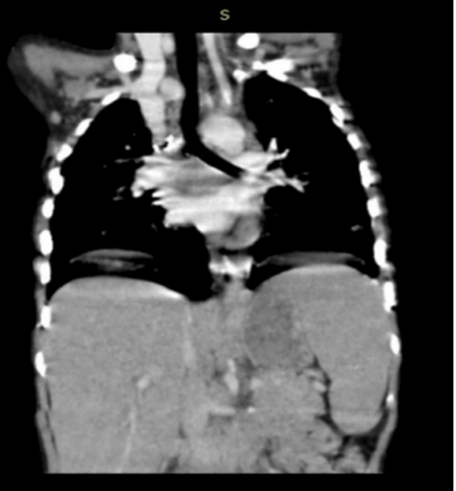
An incidental finding was seen at the lower sides of the CT abdomen, revealing filling defects seen in the segmental branches located in pulmonary arteries. CT pulmonary angiography was also done which showed cardiomegaly with filling defects in segmental branches present in pulmonary arteries (Figure 1). These findings were due to pulmonary embolism.
Figure 1. HRCT showing filling defects in segmental branches of the pulmonary arteries.
Echocardiography showed non-function right SP shunt. Large VSD with BD shunt, large ASD II with BD shunt. Severe PS with dilated and hypertrophied right ventricle and normal functioning right ventricle.
Thromboembolic disorder was suspected, plasma protein C (123%) and protein S (96%). Antithrombin III (109%) was in the normal ranges.
Possibility of post COVID thromboembolism was raised and COVID antibodies, COVID PCR, samples of serum ferritin, LDH, and D-Dimer levels were sent. The patient was diagnosed with Multisystem Inflammatory Syndrome in Children (MIS-C) because of elevated blood ferritin, LDH, and D-Dimer levels, as well as positive COVID antibodies.
Management:
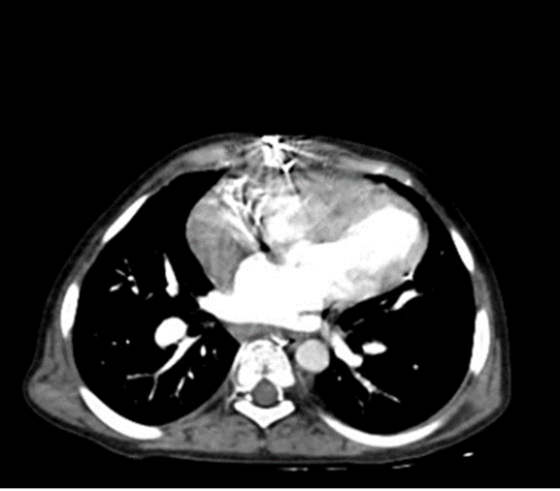
Initially, the Injection of Enoxaparin 1 mg/kg was given BD subcutaneously and monitored for Respiratory symptoms, the patient's LFTs were repeated and showed improvement with decreasing Total bilirubin and direct bilirubin and SGPT, and HRCT was repeated after 15 days. There was Significant interval reduction of pulmonary emboli (Figure 2).
Figure 2. Significant interval reduction of pulmonary arteries with reduction of pulmonary embolism.
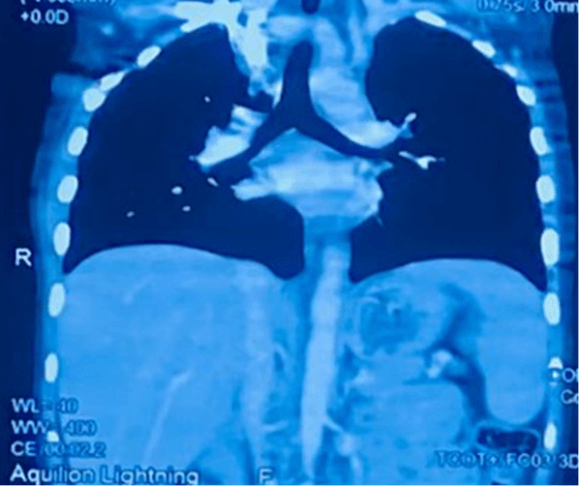
The Patient was discharged on Tab rivaroxaban for 6 weeks and follow-up HRCT was repeated, in which no filling defects were seen in the right and left main pulmonary arteries and right segmental branches (Figure 3).
Figure 3. Previously mentioned multiple filling defects not seen in scan.
 | | | | Discussion | Children with corona virus have been accounted for to be asymptomatic or with mild symptoms clinically contrasted with adults. As of late, cases of more older school-aged children and teenagers have been reported with prolonged fever, shock, pain in the abdomen, and cardiac issues after the virus that can mimic Kawasaki Disease (KD). It appears to be a hyper inflammatory illness involving several organs. The CDC (Centers for Disease Control and Prevention) has named the condition MIS-C related to corona virus and developed an example case for this disease.4,5
A young adult of age less than 21 years who claims to have had a fever for more than 24 hours, >38.0°C; laboratory reports suggesting inflammation, such as an elevated CRP (C-reactive protein), ESR (erythrocyte sedimentation rate), fibrinogen, procalcitonin, d-dimer, ferritin, LDH (lactic acid dehydrogenase), or IL-6 (interleukin 6); raised neutrophils, decreased lymphocytes, and reduced albumin; and proof of serious disease clinically that makes hospitalization necessary, with more than 2 organs involved, which can be one of the following: heart, kidney, lungs, blood and lymph nodes, gastrointestinal tract, skin, or brain and spinal cord; and no alternative conceivable diagnosis.6
The goal is to attain an anti-Xa activity level after a 4-hour dose of 0.2 to less than 0.5 U/mL. The most suitable choice in children admitted because of illness linked with COVID-19, including MIS-C, is subcutaneous low-dose low-molecular-weight heparin given two times a day for anticoagulant thromboprophylaxis in clinically stable patients without significant kidney dysfunction and without any contraindications. Unfractionated heparin should be constantly pumped intravenously in patients with severe kidney impairment, with a target to attain anti-Xa activity levels between 0.1 and less than 0.35 U/ml.7,8
Platelet count of less than 20,000 to 50-000/μL, hypofibrinogenemia (such as fibrinogen activity less than 100 mg/dL by Clauss method), an event of significant bleeding, and the consumption of aspirin at a dose higher than 5 mg/kg/d are all warning signs that the patient might have a massive bleeding risk when taken with thromboprophylaxis of anticoagulation. However, in scenarios where there are no other bleeding risk variables, low-dose thromboprophylaxis anticoagulation therapy aspirin given at doses less than or equal to 5 mg/kg/d due to heart-related abnormalities or features associated with Kawasaki-like illness is not linked to any major bleeding risk in MIS-C.7
| | | | Conclusion | | MIS-C, which is occasionally observed in the younger population, has also been noticed in patients suffering from Corona virus. Further investigation is required for the association between MIS-C and the SARS-Cov-2 infection. As knowledge and cases regarding COVID-19 in children are emerging, reporting these cases is essential to helping health care professionals identify the MISc symptoms better. This is crucial for the initiation of timely and appropriate treatment for this disease. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Nikolopoulou GB, Maltezou HC. COVID-19 in Children: Where do we Stand? Arch Med Res. 2022 Jan;53(1):1-8. doi: 10.1016/j.arcmed.2021.07.002. Epub 2021 Jul 6. PMID: 34311990; PMCID: PMC8257427. [CrossRef]
- Wichmann D, Sperhake JP, Lütgehetmann M, et al. Autopsy Findings and Venous Thromboembolism in Patients With COVID-19: A Prospective Cohort Study. Ann Intern Med. 2020;173(4):268-277. doi:10.7326/M20-2003. [CrossRef]
- Ali MAM, Spinler SA. COVID-19 and thrombosis: From bench to bedside. Trends Cardiovasc Med. 2021 Apr;31(3):143-160. doi: 10.1016/j.tcm.2020.12.004. Epub 2020 Dec 16. PMID: 33338635; PMCID: PMC7836332. [CrossRef]
- Yasuhara J, Kuno T, Takagi H, Sumitomo N: Clinical characteristics of COVID-19 in children: a systematic review. Pediatr Pulmonol. 2020, 55:2565-2575. 10.1002/ppul.24991. [CrossRef]
- https://www.cdc.gov/kawasaki/index.html
- Radia T, Williams N, Agrawal P, Harman K, Weale J, Cook J, Gupta A. Multi-system inflammatory syndrome in children & adolescents (MIS-C): A systematic review of clinical features and presentation. Paediatr Respir Rev. 2021 Jun;38:51-57. doi: 10.1016/j.prrv.2020.08.001. Epub 2020 Aug 11. PMID: 32891582; PMCID: PMC7417920. [CrossRef]
- Goldenberg NA, Sochet A, Albisetti M, et al. Consensus-based clinical recommendations and research priorities for anticoagulant thromboprophylaxis in children hospitalized for COVID-19-related illness. J Thromb Haemost. 2020;18(11):3099-3105. doi:10.1111/jth.15073. [CrossRef]
- Schmitz AH, Wood KE, BurghardtEL, et al. Thromboprophylaxis for children hospitalized with COVID-19 and MIS-C. Res Pract Thromb Haemost. 2022;6:e12780. doi: 10.1002/rth2.12780. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2026.5
|
| Cite this article as: | | qadeer A, Ally K, Waseem H, Rajani H, Khan A M. Multi system inflammatory syndrome in children (MISC) - an Incidental finding. Pediatr Oncall J. 2024 Feb 26. doi: 10.7199/ped.oncall.2026.5 |
|