Gabriela Etzel Gomes de Sa1, Miguel Machado Carlos Lopes2, Raquel Alexandra Barbosa de Nunes Gouveia Lopes2, Isabel Sampaio2, Maria da Graça Rocha Oliveira2, Rita Espírito Santo2, Maria João Palaré2.
1Faculdades Pequeno Príncipe, Curitiba, PR, Brasil,
2Departamento de Pediatria do Centro Hospitalar Universitário Lisboa Norte, EPE, Lisboa, Portugal.
ADDRESS FOR CORRESPONDENCE
Gabriela Etzel Gomes de Sá, : Rua Ângelo Nabosne, 75, ap 803.
Email: gabrielaegsa@hotmail.com | | Abstract | Introduction: Neonatal thrombosis affects approximately 3 to 5 out of every 100,000 newborns, with a mortality rate of 2 to 4%. Its occurrence may be associated with conditions involving the mother and the fetus/newborn and/or related to the medical assistance.
Case description: A full-term newborn (NB) of biamniotic bicorionic twin pregnancy, with excellent adaptation to extrauterine life, presented sudden hematuria at 28 hours of life, evolving with the need for invasive ventilation and hemodynamic support. Abdominal ultrasound revealed extensive venous thrombosis affecting the infrahepatic inferior vena cava and common iliac veins. The anatomopathological study of the placenta revealed the presence of an intervillous thrombus measuring 1.5 centimeters. The thrombotic condition was managed by the use of subcutaneous Enoxaparin and hospital discharge occurred after 45 days of hospitalization.
Discussion: The thrombus found in the intervillous space of the placenta suggests that it was the result of a maternal coagulative response as a result of a disturbance in maternal-fetal blood flow. Therefore, we believe that the thrombus found in the NB has the same origin as the thrombus found in the placenta, suggesting that the placental intervillous coagulation product has migrated to the fetal circulation. It is recommended to start the investigation of neonatal venous thrombosis through Doppler ultrasound. With regard to treatment, the agents of choice are low molecular weight heparins (LMWH), especially subcutaneous Enoxaparin sodium. It is understood that the mother-fetus binomial faced hemodynamic disorders, however, etiopathogenic clarifications are still lacking to define the triggering factor of the coagulation dysfunction. | | | | Keywords | | Venous thrombosis, newborn, enoxaparin | | | | Introduction | Neonatal thrombosis is defined by the occurrence of a thrombus occluding a blood vessel, being it a vein or an artery in a newborn (NB).1 In recent years, the incidence of thrombotic events in NBs has been increasing as a result of diagnostic advances. of this pathological condition in this period.2 Excluding the occurrence of Cerebral Vascular Accident (CVA), it is estimated that the incidence of thrombosis in neonates is around 2.5 to 15 per 1000 babies admitted to neonatal intensive care units (NICU), and 3 to 5 NBs per 100,000 births. Furthermore, it is estimated that 2 to 4% of these NBs die directly as a result of the thrombosis.1,3,4
Its occurrence in NBs may be associated with the immaturity of the coagulation system of these babies, as they have reduced levels of anticoagulants, as well as lower levels of fibrinolytic components. In addition, the occurrence of neonatal thrombosis is associated with risk factors inherent to the baby, as well as maternal risk factors, related to childbirth and the care process of health care for newborns.2,3,5
The main risk factors associated with the development of neonatal thrombosis include maternal factors such as primiparity, infertility, thrombophilia and autoimmune diseases, placental thrombosis, comorbidities (diabetes mellitus, dyslipidemia, preeclampsia), intrauterine growth restriction (IUGR), prolonged rupture and/or premature birth of ovular membranes and placental abruption, as well as neonatal factors, being the main ones the use of central catheters, sepsis, perinatal asphyxia, medications (e.g. corticosteroids), comorbidities (liver dysfunction, kidney disease, congenital heart disease, polycythemia, thrombophilia), among others. In addition, risk factors related to childbirth are also highlighted, such as emergency cesarean section, shoulder dystocia, changes in fetal heart rate and instrumented delivery.1,2,3,4,5
| | | | Case Report | Male newborn, son of a 32-year-old mother, with two previous pregnancies and history of infertility. The current pregnancy resulted from the implantation of two previously frozen embryos. No comorbidities were mentioned. During the gestational period, the mother was using acetylsalicylic acid (ASA), iodine and folic acid. Prenatal records showed immunity to toxoplasmosis and cytomegalovirus, other serologies and infectious screening were negative. Screening for gestational diabetes mellitus was also negative. Paternal age of 36 years old, without comorbidities. There is no history of consanguinity or morbid family history relevant to the case.
First twin of biamniotic bicorionic twin gestation, born by elective cesarean delivery, with gestational age of 37 weeks and 1 day. The NB's anthropometric measurements were adequate for the gestational age. The apgar score was 10 in the first minute of life and 10 in the fifth minute, with excellent spontaneous adaptation to extrauterine life. The physical examination showed no alterations. No macroscopic changes were noted in the placenta or umbilical cord. The placenta was sent for anatomopathological study.
At 28 hours of life (D2 of life), the NB presented macroscopic hematuria with the presence of clots associated with paleness, jaundice, tachypnea, signs of poor peripheral perfusion and abdomen without palpable masses. He was referred to the Neonatal Intensive Care Unit (NICU), with significant hemodynamic deterioration requiring cardiorespiratory support with invasive ventilation and vasoactive drugs.
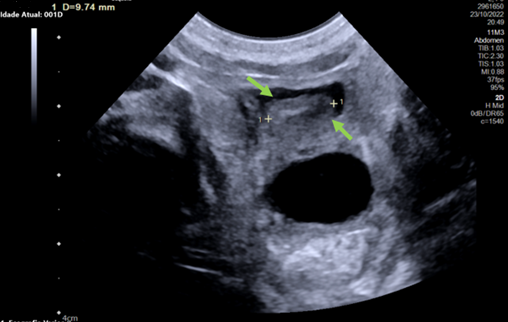
Laboratory tests revealed the presence of anemia, lactic acidosis, thrombocytopenia, elevated inflammatory activity tests and compromised renal function. Chest X-rays and transfontanellar ultrasound were performed, which showed no alterations. Abdominal ultrasound confirmed the presence of echogenic content in the lumen of the infrahepatic inferior vena cava and both common iliac veins, with no color Doppler signal at these levels, suggestive of extensive venous thrombosis (Figures 1 and 2).
Figure 1. Doppler flow interruption in the inferior vena cava due to a thrombus.
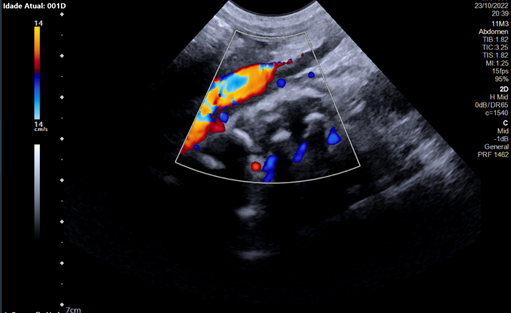
Figure 2.Visible thrombus inside the inferior vena cava measuring nine millimeters.
Therapy with subcutaneous enoxaparin was started on the same day. In the view of positive infectious parameters and multisystemic involvement, ampicillin and cefotaxime were started. At 42 hours of life (D3), the clinical picture worsened with severe metabolic acidosis with hyperlactatemia, acute kidney injury, anemia and thrombocytopenia. The blood culture was negative.
The control abdominal ultrasound revealed the persistence of signs of extensive thrombosis of the IVC and bilateral common iliac veins and probable caudal extension to the right internal iliac vein and superior portion of the right external iliac vein, with involvement of the bilateral renal veins, umbilical vein thrombosis and hepatosplenomegaly On D7, there was clinical and laboratory improvement. On D21 of life, a new abdominal ultrasound showed a reduction in the dimensions of the thrombus in the IVC and in the renal veins, as well as resolution of the hepatosplenomegaly. The diagnostic investigation was complemented with metabolic screening, chromatography of organic acids in urine and aminoacids in blood and urine, study of prothrombotic factors in the mother and baby, which did not reveal abnormalities relevant to the case. The NB remained hospitalized up to 45 days of life until reaching significant weight gain.
The anatomopathological study of the placenta revealed the presence of an intervillous thrombus measuring 1.5 centimeters in its longest axis, with no other alterations. In the placenta of the other twin, which did not show thrombotic clinical manifestations, a hemorrhagic area was identified adjacent to the insertion of the membranes of the fetal face, as well as a hematoma on the maternal face. No other alterations were described in the examination report.
| | | | Discussion | It is suggested that venous thromboembolism in pediatric patients is mainly caused by the association of at least two prothrombotic risk factors and result in longer hospitalization, manipulation of central catheters and increased risk of bleeding due to the institution of anticoagulant therapy.2,6 The reported case describes a male NB, born at term without intercurrences, resulting from in vitro fertilization (IVF) of frozen embryos from a mother with a history of infertility, however, without any other aspects that suggest the etiopathology of thrombosis.
Later in the investigation, the study of the placenta revealed the presence of an intervillous thrombus with 1.5 cm, with no other alterations. The intervillous space is occupied by maternal blood and ensures adequate fetal gas exchange. In this sense, disturbances of this blood flow result in a maternal coagulative response.7,8 Given the above, we believe that the thrombus found in the NB has the same origin as the thrombus found in the placenta, suggesting that the placental intravillous coagulation product has migrated to the fetal circulation of the affected twin.
A single-center retrospective cohort study conducted in the United States demonstrated that acute and chronic placental injuries often accompany neonatal thrombotic conditions, with 90% of neonatal stroke cases having at least one placental abnormality. The study reinforces that inflammatory conditions of the placenta, mainly fetal asphyxia and maternal infection, contribute to the formation of a placental embolus that subsequently reaches the fetal circulation.9
Regarding the pathophysiology of thrombosis, Virchow's triad describes three important components of thrombus formation – hypercoagulability, endothelial injury, and abnormal blood flow.8 In order to determine whether placental changes occur as a result of thrombus formation, an American experimental study carried out with mice suggested that damage to the placental vasculature after exposure to intrauterine inflammatory conditions may result in blood flow stagnation and, consequently, vascular damage. Thus, in addition to hypercoagulability, translated by the gestational period itself, changes in blood flow resulting from the intrauterine inflammatory environment and possible endothelial damage represent the second and third pillars of Virchow's triad.10,11
Regarding the diagnostic approach, it is recommended to start the investigation of babies with venous thrombosis through Doppler ultrasound, which is the first-line imaging exam, in addition to the anatomopathological study of the placenta and minimally invasive laboratory tests, such as blood count, coagulogram (PT, TT, a PTT, fibrinogen and D-dimer), protein C, protein S, antithrombin, lupus anticoagulant, anti-cardiolipin antibodies, anti-beta 2-glycoprotein 1 antibodies, factor V Leiden, prothrombin G20210A genetic mutations and Von Willebrand factor (vWF) research.2,3
With the aim of preventing the development of embolism and restoring blood flow interrupted by thrombosis, the agents of choice for treatment are low molecular weight heparins (LMWH), especially Enoxaparin sodium, which should be administered at a dose of 1.5 to 1.7 mg/kg, subcutaneously, every twelve hours, for 6 weeks to three to six months, according to the 2022 Neonatal Thrombosis Consensus of the Portuguese Society of Neonatology, still under public discussion. Monitoring should be performed with measurement of anti-Xa levels approximately four hours after administration of the second dose of LMWH and weekly thereafter. Unfractionated heparin (UFH) is an alternative when LMWH is unavailable, but it can only be used in cases where antithrombin levels are adequate, in addition to having a short half-life and variable bioavailability. A major advantage of using LMWH compared to UFH is the reduction in platelet factor IV and osteoblasts, reducing the risk of heparin-induced thrombocytopenia and osteopenia.2
Despite its rare occurrence and, mainly, its little-described presentation regarding risk factors and etiologies, fortunately, the described case was successfully managed through high clinical suspicion and the use of effective and efficient diagnostic methods, such as ultrasonography, as well as through subcutaneous therapy with Enoxaparin. There are still etiopathogenic clarifications to be made in order to define the triggering factor of coagulation dysfunction in the placenta and in the affected twin. It is hoped that sharing the experience acquired with the management of this case will serve as a subsidy for new perspectives and research on neonatal thrombosis. The importance of disseminating information on rare cases of neonatal thrombosis is also highlighted, so that more studies on this pathological condition can be directed, mainly regarding etiological investigation and prevention. The hypothesis arises that there may be conditions or situations that lead to the occurrence of thrombosis in newborns that are still unknown by the scientific community. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Robinson V, Achey MA, Nag UP, et al. Thrombosis in infants in the neonatal intensive care unit: Analysis of a large national database. J Thromb Haemost. 2021;19(2):400-7. [CrossRef]
- Makatsariya A, Bitsadze V, Khizroeva J, et al. Neonatal thrombosis. J Matern Neonatal Med. 2022;35(6):1169-77. Available from: https://doi.org/10.1080/14767058.2020.1743668. [CrossRef]
- Sociedade Portuguesa de Neonatologia. Consenso clínico "Trombose Neonatal". Portugal, 2022.
- Bhatt MD and Chan AKC. Venous thrombosis in neonates. Faculty Reviews 2021 10:(20). Available from: https://doi.org/10.12703/r/10-20. [CrossRef]
- Kenet G, Cohen O, Bajorat T, et al. Insights into neonatal thrombosis. Thromb Res [Internet]. 2019; 181(March):S33-6. Available from: https://doi.org/10.1016/S0049-3848(19)30364-0. [CrossRef]
- Bhat R, Kumar R, Kwon S, et al. Risk Factors for Neonatal Venous and Arterial Thromboembolism in the Neonatal Intensive Care Unit-A Case Control Study. J Pediatr [Internet]. 2018; 195:28-32. Available from: https://doi.org/10.1016/j.jpeds.2017.12.015. [CrossRef]
- Sukhanova M, Mithal LB, Otero S, et al. Maternal vs Fetal Origin of Placental Intervillous Thrombi. Am J Clin Pathol. 2022; 157(3):365-73. [CrossRef]
- Arêas ALBG, Neto ARB. Patologia Geral. Capítulo 10: Patologia Feto Placentária. Sociedade Brasileira de Patologia. São Paulo - SP, 2022.
- Leon RL, Kalvacherla V, Andrews MM, et al. Placental pathologic lesions associated with stroke in term neonates. Front Endocrinol (Lausanne). 2022; 13 (September): 1-9. [CrossRef]
- Lowe GDO. Virchow's Triad Revisited. 2004;109 (February): 213-5.
- Eloundou SN, Lee JY, Wu D, et al. Placental malperfusion in response to intrauterine inflammation and its connection to fetal sequelae. PLoS One. 2019; 14(4):1-15. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2026.18
|
| Cite this article as: | | Sa G E G d, Lopes M M C, Lopes R A B d N G, Sampaio I, Oliveira M d G R, Santo R E, Palaré M J. Inferior vena cava and common iliac thrombosis in a newborn twin. Pediatr Oncall J. 2024 Mar 04. doi: 10.7199/ped.oncall.2026.18 |
|