Filipa Sutre, Margarida Caldeira, Alexandra Gavino, Aldina Lopes.
Paediatric Department, Hospital de Santarém, Santarém, Portugal.
ADDRESS FOR CORRESPONDENCE
Filipa Sutre, Pediatric Department, Hospital de Santarém, Avenida Bernardo, Santareno 3737B, 2005-177 Santarém, Portugal.
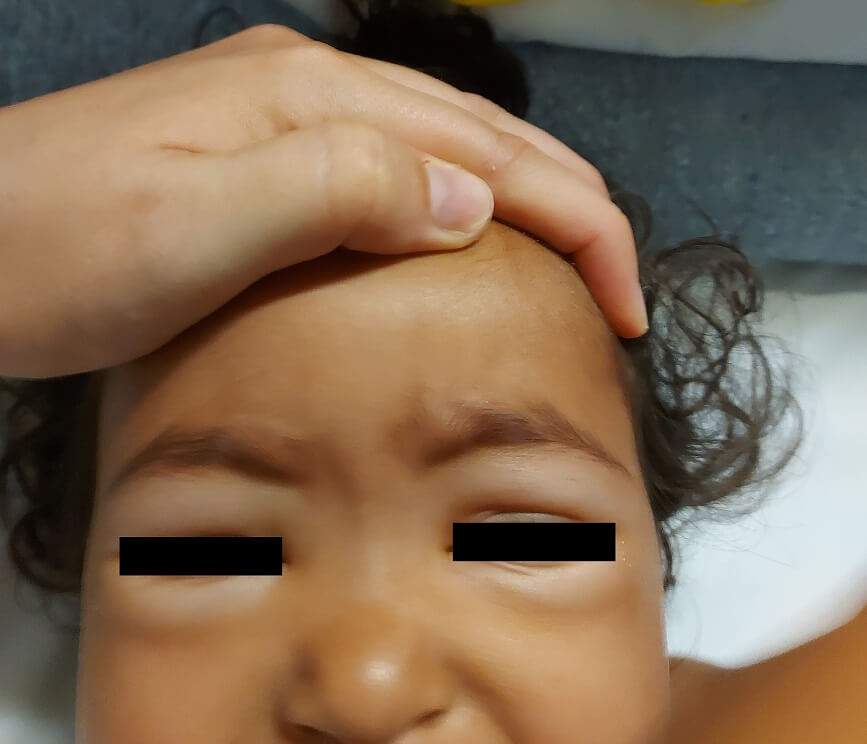
Email: filipasutre@gmail.com | | Abstract | | Giardiasis, caused by Giardia lamblia, is an intestinal infection that presents various clinical manifestations. While malabsorption is a recognized complication, protein-losing enteropathy (PLE) is infrequent. This report describes a 17-month-old healthy girl who presented to the emergency department exhibiting generalized edema attributed to hypoalbuminemia, which resulted from gastrointestinal protein loss. Subsequent investigations identified giardiasis as the underlying etiology. After appropriate treatment, the patient fully recovered. With this case, the intention is to highlight the importance of considering giardiasis in patients with hypoproteinemia of unknown origin to prevent severe comorbidities, particularly in children. | | | | Keywords | | Hypoalbuminemia, Giardiasis, Protein-Losing Enteropathy. | | | | Case Report | A 17-month-old healthy girl of Indian descent, following a vegetarian diet and maintaining adequate nourishment, experienced a mild febrile illness with watery diarrhea and vomiting two weeks before seeking admission to the emergency department. One week later, she developed facial edema, as shown in Figure 1, hands and feet, without other associated symptoms. The physical examination revealed the patient to be afebrile with stable vital signs; however, she exhibited pallor in the skin, diffuse pitting edema and abdominal distention, with no signs of organomegaly. The chest X-ray displayed no abnormalities and the abdominal ultrasound indicated a small quantity of free intraperitoneal fluid in the subhepatic and perisplenic regions. Laboratory findings revealed anemia (hemoglobin 10.8 g/dL), hypoproteinemia (2.9 g/dL) and hypoalbuminemia (1.4 g/dL). Serum biochemical parameters for liver and kidney function were within the normal range. Urinalysis and a 12-hour urinary protein excretion test excluded the presence of proteinuria. Additionally, ferritin, calcium, vitamin D and serum levels of immunoglobulin G were found to be low. Celiac disease was eliminated from the diagnostic considerations. Despite stool cultures failing to identify pathogenic organisms, the stool analyses for Giardia lamblia antigen consistently yielded positive results in three samples. She underwent management with fluid restriction and a high-protein diet supplemented with iron, calcium and vitamin D. Following a five-day albendazole treatment, there was a remarkable improvement in signs, symptoms and laboratory findings. One month after being discharged, during her follow-up visit, she remained asymptomatic; the physical examination was completely normal and her serum levels of total protein, albumin and immunoglobulins were within the normal range.
Figure 1. Facial edema.
| | | | Discussion | Giardiasis, caused by the extracellular protozoan parasite Giardia lamblia, is a worldwide intestinal infection.1 The symptoms of giardiasis can manifest across a spectrum of severity, encompassing asymptomatic instances to more pronounced presentations, which may involve acute or chronic diarrhea, nausea, bloating, abdominal pain and weight loss.2 While malabsorption is an acknowledged complication of Giardia infection, selective protein-losing enteropathy (PLE) is uncommon. In instances of severe hypoproteinemia, symptoms may involve edema, ascites, pericardial or pleural effusion or a combination and may also be linked to an elevated susceptibility to infections.3 Our patient exhibited generalized pitting edema with ascites but without pleural or pericardial effusion.
PLE is characterized by the pronounced loss of proteins through the gastrointestinal tract, occurring when the losses into the gastrointestinal system surpass the liver's production capacity.3,4 The leakage of serum proteins into the gastrointestinal tract occurs independently of molecular weight. Consequently, the serum proteins most affected by this disrupted equilibrium are those with extended half-lives, such as immunoglobulin A (IgA), IgG, IgM, albumin, fibrinogen and ceruloplasmin.4 In our patient, there was evidence of hypoalbuminemia and reduced levels of serum IgG.
The consideration of PLE in patients presenting with hypoproteinemia is warranted after excluding other potential causes, such as insufficient dietary intake, significant proteinuria, impaired protein synthesis due to liver disease, obstruction in the lymphatic system and extensive inflammation of the vasculature (as seen in sepsis).3 PLE was suspected in this patient due to the simultaneous presence of gastrointestinal signs and symptoms without the occurrence of proteinuria or clinical and laboratory evidence of liver disease. The patient's vegetarian diet could contribute to an inadequate dietary intake of protein and energy. However, isolated vegetarianism is rarely associated with such low albumin levels, as observed in our patient.
Despite significant advancements in recent decades in elucidating the pathogenesis of giardiasis, the pathophysiology of this disease remains a subject of ongoing investigation.5 It is hypothesized that Giardia lamblia colonizes the upper part of the small intestine, specifically the duodenum and jejunum, without invading the tissues. This colonization can result in damage to the intestinal mucosa, compromising the barrier function of enterocytes by disrupting the epithelial brush border and tight junctions.2,5 This leads to malabsorption, resulting in clinical manifestations such as anorexia, abdominal pain, diarrhea and weight loss. Consequently, patients may experience various deficiencies in minerals and vitamins, including iron, folic acid, vitamin B12, vitamin A and thiamine, leading to anemia.5 The deficiency in iron is a widely acknowledged complication associated with giardiasis, in line with the existing literature.6 Our patient manifested abdominal distention and edema, indicative of malabsorption. Additionally, she exhibited anemia, low serum ferritin levels, vitamin D deficiency and low calcium levels. These conditions might be linked to insufficient dietary intake, malabsorption or a combination of both, requiring supplementation.
Regarding the diagnosis, molecular tests utilizing enzyme-linked immunosorbent assay (ELISA) to detect Giardia lamblia antigens demonstrate high specificity and sensitivity, making them a recommended choice for initial diagnostic testing.3 In a comparative analysis, the effectiveness of microscopic examination of stool samples for parasites was reported as 83%, while stool antigen tests showed a higher sensitivity at 95%.7 In our patient, even though stool cultures did not identify pathogenic organisms, ELISA for detecting Giardia lamblia antigen consistently yielded positive results in three samples.
Giardia lamblia can induce illness both during the acute phase of the infection and in the post-infectious period. Evidence from a prospective longitudinal cohort study indicates that giardiasis in early life was identified as a risk factor for stunted growth at two years of age.2,8 Therefore, despite PLE being considered a rare manifestation of giardiasis, its identification is crucial and eradicating the infection leads to rapid recovery, as evidenced in our patient.
In conclusion, giardiasis is a treatable cause of PLE, potentially linked to severe comorbidities. Conducting an epidemiological investigation and promptly recognizing and treating Giardia infection in PLE cases contribute to swift clinical and laboratory recovery. This approach is crucial for preventing malnutrition, particularly in growing children. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Feng, Y., & Xiao, L. (2011). Zoonotic potential and molecular epidemiology of Giardia species and giardiasis. Clinical microbiology reviews, 24(1), 110-140. https://doi.org/10.1128/CMR.00033-10. [CrossRef]
- Allain, T., & Buret, A. G. (2020). Pathogenesis and post-infectious complications in giardiasis. Advances in parasitology, 107, 173-199. https://doi.org/10.1016/bs.apar.2019.12.001. [CrossRef]
- Akkelle, B. S., Tutar, E., Sengul, O. K., et al. (2018). A Rare Complication of Giardiasis in Children: Protein-losing Enteropathy. The Pediatric infectious disease journal, 37(12), e345-e347. https://doi.org/10.1097/INF.0000000000002025. [CrossRef]
- Takeda, H., Ishihama, K., Fukui, T., et al. (2003). Significance of rapid turnover proteins in protein-losing gastroenteropathy. Hepato-gastroenterology, 50(54), 1963-1965.
- Allain, T., Amat, C. B., Motta, J. P., et al. (2017). Interactions of Giardia sp. with the intestinal barrier: Epithelium, mucus, and microbiota. Tissue barriers, 5(1), e1274354. https://doi.org/10.1080/21688370.2016.1274354. [CrossRef]
- De Vizia, B., Poggi, V., Vajro, P., et al. (1985). Iron malabsorption in giardiasis. The Journal of Pediatrics, 107(1), 75-78. https://doi.org/10.1016/s0022-3476(85)80618-1. [CrossRef]
- Addiss, D. G., Mathews, H. M., Stewart, J. M., et al. (1991). Evaluation of a commercially available enzyme-linked immunosorbent assay for Giardia lamblia antigen in stool. Journal of Clinical Microbiology, 29(6), 1137-1142. https://doi.org/10.1128/jcm.29.6.1137-1142.1991. [CrossRef]
- Donowitz, J.R., Alam, M., Kabir, M., et al. (2016). A Prospective Longitudinal Cohort to Investigate the Effects of Early Life Giardiasis on Growth and All Cause Diarrhea. Clin Infect Dis. 15;63(6):792-7. doi: 10.1093/cid/ciw391. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2026.65
|
| Cite this article as: | | Sutre F, Caldeira M, Gavino A, Lopes A. Protein-Losing Enteropathy as a Rare Complication of Giardiasis in Children. Pediatr Oncall J. 2026;23. doi: 10.7199/ped.oncall.2026.65 |
|