Ali Kumble, Abhishek K Phadke, Arun Varghese, Poonam Raikar, Kaushal Patel, Shuhada Arif Khan.
Indiana Hospital and Heart Institute, Mangaluru, Karnataka, India.
ADDRESS FOR CORRESPONDENCE
Poonam Raikar, Consultant pediatrician and neonatalogist, Indiana Hospital and Heart Institute, Mangaluru, India.
Email: drpoonamvernekar@gmail.com | | Abstract | Background: midazolam is the most widely used agent in procedural sedation. The objective of the study was to compare the efficacy of midazolam administered via intranasal and intravenous route among pediatric patients.
Methods: An open-labeled randomized controlled trial was conducted in a tertiary care hospital. Children between six months and 10 years requiring sedation for investigative procedures (both invasive and noninvasive) were randomly assigned to either intranasal group (0.2 mg/kg body weight) or via intravenous group (0.1 mg/kg body weight). The main outcomes measured were mean time taken for sedation, level and adequacy of sedation and ease of doing procedure between the two groups. The secondary outcome measures included the number of doses required, procedure completion rate and the total number of adverse events between the two groups respectively.
Results: 44 patients (22 in each group) were enrolled over a 9-month study period. Mean time (in minutes) taken for satisfactory sedation by intravenous route was 5.5 ± 2.31 as compared to 10.29 ± 1.72 in intranasal route (P = 0.001). The frequency of oxygen desaturation was more in intravenous group as compared to intranasal group. The rest of the measured variables were similar in both the groups with no statistical difference between the groups.
Conclusion: midazolam administered via intravenous route had shorter mean time of sedation albeit with more adverse events than intranasal route. If time taken for intravenous administration is added, intranasal route is easier and faster. Both the routes were comparable. | | | | Keywords | | Anxiety, Children, midazolam, Procedural Sedation. | | | | Introduction | Children are more prone to anxiety during their visit to a healthcare setting that gets exacerbated by routine procedures (both invasive and non-invasive) during investigation and appropriate management.1 Feeling afraid or anxious while engaging with clinicians is not uncommon among children.2 They often respond via behavior instead of words to communicate what they feel that include aggression, withdrawal, lack of cooperation and regression.3 These emotional responses can delay important medical treatment, take more time to complete investigation procedure and reduce patient satisfaction.4
Coaxing and physical restraint may not be appropriate since it might make the procedure difficult and unsafe for the child with psychological consequences.5 Effective management of anxiety in pediatric patient improves outcomes as well as patient cooperation and parental satisfaction.6 With growing trends in medical sciences, clinicians now have a large armamentarium of drugs with which they can calm the pediatric patient and ease the discomfort of unpleasant procedure.7
Adequate sedation and anxiolysis is integral part of successful and smooth procedure completion. Many professional bodies have outlined definitions and guidelines of sedation8 eventually replacing the term ‘conscious sedation’ with’ procedural sedation’.9 Procedural sedation refers to the technique of administering sedatives or dissociative agents with or without analgesics to induce an altered state of consciousness that allows the patient to tolerate painful or unpleasant procedures while preserving cardiorespiratory function.10 With procedural sedation emerging as a new skill set, different pharmacological agents are being used while simultaneously considering the goals of procedural anesthesia.11
Benzodiazepines are frequently used as sedative agents that are safe and short acting in pediatric patients. midazolam is a water soluble benzodiazepine that is short acting with excellent safety record as compared to diazepam and lorazepam in recommended doses.12 It can be administered via intravenous, intramuscular, oral, rectal and intranasal route with proven efficacy and safety.13 Intranasal route is non-invasive easy to administer with good absorption, bioavailability and rapid onset of therapeutic effect owing to greater permeability of nasal mucosa. The low metabolic environment of nose overcomes the limitation of oral route and duplicates intravenous administration.14
Pediatric procedural sedation is a grey area with guidelines issued based on expert opinions that are not uniformly accepted. The paucity of data on pediatric procedural sedation in an Indian setting that evaluated midazolam as the drug of choice using two different routes of administration, prompted us to conduct the present study. The objective of the study was to compare the efficacy of midazolam via intranasal route and intravenous route for procedural sedation among children aged 6 months to 10 years. We hypothesized that midazolam is equally effective and safe by intranasal route in comparison to intravenous route.
| | | | Methods & Materials | Study Design and Setting
A hospital based, prospective, open-labeled, randomized controlled study was conducted from March 2019 to December 2019 in Department of Pediatrics at a Multi-specialty tertiary care center. The study was approved by Institutional Ethical Committee.
Study participants
A sample size of 44 patients (22 in each group) was calculated based on 95% confidence interval, 5% allowable error, with a power of 90% and quantitative data obtained from a previous study.15 Patients reporting to the Department of Pediatrics formed the target population and patients in the age group of six months to 10 years were considered in the sampling frame. Patients were enrolled as study participants from the sampling frame after fulfilling the inclusion and exclusion criteria which are as follows:
Inclusion criteria:
● Parents of patients providing informed consent.
● Patients reporting to Outpatient Department (OPD) and Inpatient Department (IPD) for diagnostic and therapeutic procedure that can be performed outside operating room requiring sedation as defined in methodology.
Exclusion criteria:
Parents of patients who refused to provide informed consent and patients having associated co-morbidities that includes, but not limited to,
● Severe respiratory distress/depression.
● Past history of adverse reaction to benzodiazepine
● Local nasal condition-nose block, severe rhinitis
● Pre procedural poor sensorium (neurological instability)
● Unstable vital due to any underlying disease process (hemodynamic instability)
Randomization and masking
Children were randomized using computer-generated block randomization with variable block sizes in 1:1 ratio to one of the two groups treated with Intranasal midazolam and intravenous midazolam. The randomization lists were kept in sequentially numbered, sealed, opaque envelopes for allocation concealment that was managed by a staff who did not reveal the randomization until the start of the study. Due to the apparent difference in the method of drug administration, the investigators were not blinded. The groups were stratified according to age groups and consisted of permuted blocks of randomly varying sizes.
Intervention and Procedure
Patients were randomized to receive either intranasal midazolam and intravenous midazolam. A routine physical examination with review of medical history and measurement of baseline vital parameters preceded administration of drug. In accordance with standard anesthesia guidelines, children underwent fasting prior to procedural sedation. The fasting protocol consisted of the following intervals: clear liquids 2 hours, breast milk 4 hours, formula feed/light meals 6 hours and heavy meals 8 hours.16 All the patients undergoing invasive procedures applied EMLA patch at the site of the procedure 30 minutes prior to procedure.
Administration of drug was done in a room with facilities to manage any emergency situation requiring resuscitation (if at all) under the surveillance of doctor well trained in these procedures. Patients in intranasal group received an aqueous intranasal spray in recommended dose of 0.2 mg/kg body weight (MIDACIP 0.5 nasal spray, Cipla) that was equally divided and administered into each nostril delivering 0.5 mg of drug per spray.17 Patients in intravenous group received a commercially available drug in recommended dose of 0.1 mg/kg body weight (prepared after appropriate dilution of 1mg/ml) administered via intravenous route over two to three minutes.
The planned procedures (both invasive and non-invasive) started as soon as the sedation reached a score of 3 (as per the Ramsay Sedation Scoring criteria) following which sedation score and vitals monitoring continued every five min throughout the procedure.
If the sedation score of three was not achieved in 20 minutes post administration, the entire procedure of drug administration was repeated up to a total of three doses failing which the procedures was categorized as failed sedation. The patient was then managed using Pediatric Intensive Care Unit (PICU) sedation protocol as per the unit’s policy. The same procedure was repeated if sedation scores dropped below than three during the procedure. In case of any adverse event, the procedure was stopped immediately and appropriate corrective steps and reversal of sedation performed and the details of event were noted down. The level of sedation was monitored till sedation level three was achieved followed by monitoring of vitals and sedation level till the procedure was completed. After the completion of procedure complications were documented on a standard form and patients were kept under observation. The sedation levels were recorded until the patient had returned to his or her baseline level of consciousness. The patients were then discharged at the discretion of attending physician after desired discharge criteria were met. Feeding was discontinued as soon as patient was enrolled in the study till they were discharged.
Outcome Measures
The main outcome measure was the comparison of level and adequacy of sedation, mean time taken for sedation and ease of doing procedure between the two groups. The secondary outcome measures included the number of doses required, procedure completion rate, failed sedation and the total number of adverse events between the two groups respectively.
Data Analysis
The data was analyzed using statistical software for windows [SPSS, version 16, SPSS Inc., USA]. For analysis, ease of doing procedures was categorized as excellent, good, satisfactory and poor. For adequacy of sedation, Ramsey Sedation Scores were regrouped into inadequate, excellent and excess sedation. Data was described using mean and standard deviation (for continuous data) and graphs (categorical data). Categorical data was analyzed using Chi-square test and continuous data was analyzed using unpaired t test. Mann Whitney U test was used to analyze ordinal data with scoring scales and the level of significance was set at P ≤0.05. | | | | Results | In the present study spanning 9 months the baseline characteristics of study participants in both the groups was similar. (Table 1) There was no statistically significant difference in the outcome measure between intranasal and intravenous group with respect to the number of doses (P=0.92), sedation score (P=0.36), ease of doing procedure (P=0.64), adequacy of sedation (P=0.80), procedure completion (P=0.71) and the prevalence of adverse events (P=0.21) respectively. (Table 2)
Table 1. Distribution of study participants according to age, gender, procedure performed and dose required for appropriate sedation.
| |
Intra-nasal group |
Intravenous group |
| Age |
|
|
| Mean Age (in years) |
3.32 ± 3.1 |
4.3 ± 2.8 |
| 6 months - <5 years |
15 (68.18) |
10 (45.45) |
| 5 years - 10 years |
7 (31.82) |
12 (54.55) |
| Gender |
|
|
| Male |
9 (40.91) |
14 (63.64) |
| Female |
13 (59.09) |
8 (36.36) |
| Procedure |
|
|
| Lumbar Puncture |
5 (22.73) |
6 (27.27) |
| Bone marrow aspiration |
1 (4.5) |
1 (4.55) |
| EEG |
3 (13.64) |
5 (22.73) |
| MRI |
8 (36.36) |
6 (27.27) |
| CT |
5 (22.73) |
4 (18.18) |
EEG-electroencephalogram; MRI-magnetic resonance imaging; CT-computerized tomography
Table 2. Comparison of the outcomes measures between Intra-nasal and Intravenous group.
| |
Intra-nasal group |
Intravenous group |
P value |
| Number of doses required |
|
|
|
| One |
11 (50) |
10 (45.45) |
P = 0.92 |
| Two |
4 (18.18) |
5 (22.73) |
|
| Three |
7 (31.82) |
7 (31.82) |
|
| Sedation Scores Achieved |
|
|
|
| Score 1 |
5 (22.73) |
3 (13.64) |
P = 0.36 |
| Score 2 |
0 |
1 (4.55) |
NS |
| Score 3 |
4 (18.18) |
9 (40.91) |
|
| Score 4 |
10 (45.45) |
5 (22.73) |
|
| Score 5 |
1 (4.55) |
2 (9.09) |
|
| Score 6 |
2 (9.09) |
2 (9.09) |
|
| Ease of doing procedure |
|
|
|
| Excellent |
2 (9.09) |
2 (9.09) |
P = 0.64 |
| Good |
6 (27.27) |
10 (45.45) |
NS |
| Satisfactory |
8 (36.36) |
6 (27.27) |
|
| Poor |
6 (27.27) |
4 (18.18) |
|
| Adequacy of Sedation |
|
|
|
| Inadequate Sedation |
5 (22.73) |
4 (18.18) |
P = 0.80 |
| Excellent Sedation |
16 (72.73) |
16 (72.73) |
NS |
| Satisfactory |
8 (36.36) |
6 (27.27) |
|
| Excess Sedation |
1 (4.55) |
2 (9.09) |
|
| Procedure completion |
|
|
|
| Successful |
17 (77.27) |
18 (81.82) |
P = 0.71 |
| Failure |
5 (22.73) |
4 (18.18) |
NS |
| Adverse events during procedure |
|
|
|
| No |
20 (90.91) |
17 (77.27) |
P = 0.21 |
| Yes |
9 (9.09) |
5 (22.73) |
NS |
Level of significance set at P = 0.05
NS-not significant using Chi-Square test
Though not significant, the frequency of adverse event was higher in the intravenous group where three study participants had SPO2 levels below 90%. (Figure 1) The mean time taken to reach sedation scores ≥3 or more was lesser in the intravenous group that was statistically significant (P=0.001) (Figure 2 and Table 3). In addition, though not significant the time taken to discharge study participants was higher in intravenous group (P=0.77) (Figure 3 and Table 4).
Figure 1. Distribution of adverse effects in both the groups (Frequency).
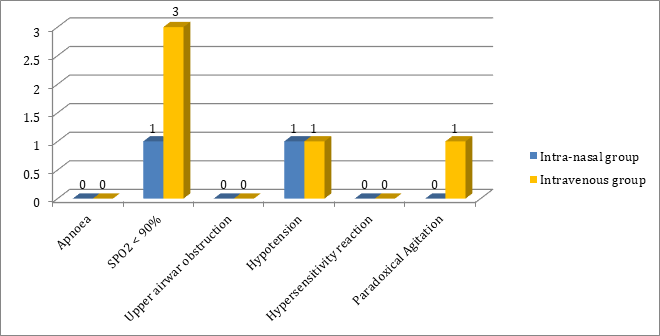
Figure 2. Mean time taken (in minutes) to reach sedition score of =3 between two groups.
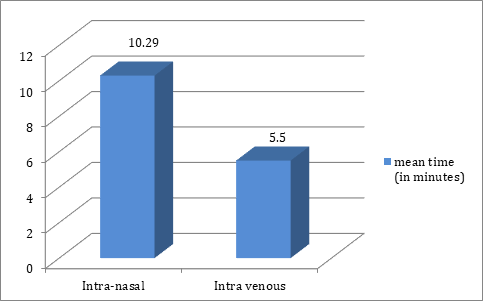
Table 3. Comparison of mean time (in minutes) taken to reach sedation score of ≥3.
| Groups |
N |
Mean ± SD |
P value |
| Intra nasal |
22 |
10.29 ± 1.72 |
P=0.001* |
| Intra venous |
22 |
5.5 ± 2.31 |
|
Level of significance at P = 0.05
*Statistically significant using Mann Whitney Test
Figure 3. Mean time taken (in minutes) for discharge after fulfillment of discharge criteria between two groups.
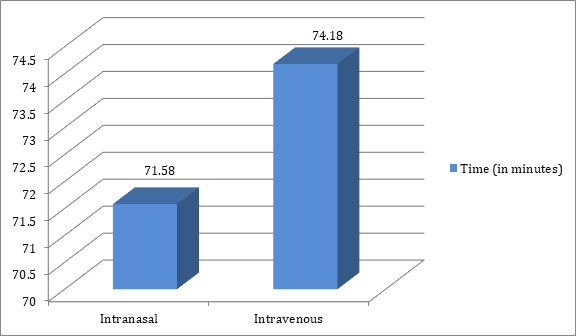
Table 4. Comparison of mean time (in minutes) for discharge after fulfillment of discharge criteria.
| Groups |
N |
Mean ± SD |
P value |
| Intra nasal |
22 |
71.58 ± 26.37 |
P = 0.772 |
| Intra venous |
22 |
74.18 ± 27.58 |
NS |
Level of significance at P = 0.05
NS-not significant using Mann Whitney Test
| | | | Discussion | In recent years there has been increasing efforts to make pediatric procedural sedation smooth and safe for children undergoing distressing procedures. In addition, the search for an ideal sedative for pediatric procedural sedation is still on, although various drugs like chloral hydrate, midazolam, ketamine, propofol and thiopentone are being used in various doses and routes, either single or in combination.9 The goal of our prospective randomized control study was to determine the efficacy of midazolam by intranasal route. The findings from this randomized trial suggest that there was no significant difference between intranasal and intravenous route for most of the parameters except the mean time taken to reach sedation score of ≥3 that was significantly less by intravenous route.
The age group preferred in the present study was between 6 months to 10 years, as less than 6 months is too young and more than 10 years children can undergo non-invasive (painless) procedure without sedation.15 The distribution of gender and the commonly performed pediatric procedures were comparable and were not significant in the present study. Sedation was sufficient in the first dose for about 50% and 45% in both the groups and another 31.8% required three doses respectively. The doses used in the present study were kept very minimal keeping in mind the safety for the patient. Nevertheless, data from previous studies reveals that reinforcing doses to achieve optimum sedation was less where higher doses of medications was used.14,15
In the present study we used Ramsey Sedation Scale to assess the level of sedation that has been found to be reliable in pediatric patients.18 Given that adequate sedation was considered with a score of ≥3, we observed that patients in intra-nasal group experienced greater depth of sedation as compared to patients in intravenous group. Intranasal administration allows for rapid absorption of sedatives into the bloodstream, resulting in faster onset and deeper levels of sedation. By avoiding first-pass metabolism, intranasal route allows more of the sedative to reach the brain and central nervous system. Intranasal administration delivers sedatives directly to the brain via the nasal mucosa, potentially leading to more intense sedation.19 These trials reported that intra-nasal midazolam is effective in children during routine emergency procedures15, had a success rate of 92% during procedural sedation in pediatric patients15 and a faster pharmacodynamics profile as compared to intramuscular route.20
The ease of doing procedure was assessed over a FOUR (Full Outline Of UnResponsiveness)
point score21 and ease of doing procedures was found to be excellent in both the groups, however, the ease of procedure was found to be good among 45.4% of patients in the intravenous group. Though not significant, it was observed that ease of procedures was poor among patients in the intranasal group as compared to intravenous group.22 Since our results were not significant, we can assume that both routes of administration had their own challenges. Intranasal route has variable absorption rates and there is difficulty in achieving accurate dosing. Administration via intranasal route also causes nasal irritation or discomfort, not a good choice in children with anatomical abnormalities of nose.23 Sometimes equipment malfunction can happen (atomizers). Intravenous sedation has slower onset of sedation, longer recovery time, increased risk of respiratory depression and hypotension. It also has higher incidence of post-procedure nausea and vomiting.24 Similarly, the adequacy of sedation and procedure completion rate was found to be similar between the two routes of administration. Given that intranasal route of administration had more MRI procedures which require longer time to complete, it points towards achieving a deeper sedation for MR imaging in pediatric patients.
We observed that intranasal midazolam was well tolerated by patients. Although there were no major episodes of respiratory or cardiovascular adverse effect in any group, oxygen desaturation and paradoxical agitation was more in intravenous group as compared to intranasal group.25 All episodes of oxygen desaturation were managed by supplementing oxygen. We concluded that safety profile of intranasal midazolam is comparable with intravenous midazolam and hence it can be safely used as procedural sedative in children.
The mean time taken for satisfactory sedation was shorter for the intravenous group than the intranasal group that was statistically significant. The mean time of 10.29 minutes for intranasal group was comparable to various studies that reported almost similar mean time.20,26,27 The intravenous group reported a mean time of 5.5 minutes that was also similar to results obtained from a previous study.25 Intravenous midazolam has shorter time of onset compare to intranasal midazolam, nevertheless if we add time that was utilized for intravenous administration, the collective time becomes faster and easier with intranasal midazolam. Our study showed no significant difference in the time taken to discharge once the discharge criteria were met by the groups. The range of 71.5 minutes (intranasal) to 74.1 minutes (intravenous) was similar to a study conducted where the mean discharge was 79 minutes15 and higher than another study with mean discharge time of 66 minutes.28
Strength
We believe this to be a pioneering study in use of intranasal midazolam as a procedural sedative in children. In addition, implementation of randomization and inclusion of most of the common pediatric (invasive and non-invasive) procedures add strength to our study design.
Limitations
Our study had a few limitations but every effort was made to minimize their effects on the study outcome. First, we could not analyze data of (invasive and non-invasive) procedure separately in both groups because of comparatively smaller sample size in terms of individual procedures in both groups. Second, though randomization was adhered too, we could not ‘blind’ the intervention due to different routes of drug administration in both groups. Ours was a resource limited setup, whereas blinding requires more numbers of trained personnel which was not possible due to limited man power.
| | | | Conclusion | | It can therefore be concluded that midazolam administered via intravenous route required lesser time to reach satisfactory level of sedation than the intranasal route. The frequency of adverse effects was more in intravenous group than in intranasal group. In addition, there were no significant differences in any of the outcome measures used in the present study that advocates any particular route of administration of midazolam. The safety profile of patient was more prominent in intranasal group. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Lerwick JL. The impact of child-centered play therapy on anxiety levels in pre-neurosurgical pediatric patients. Oregon State University;
- Lerwick JL. Psychosocial implications of pediatric surgical hospitalization. Semin Pediatr Surg. 2013 Aug;22(3):129-33. [CrossRef] [PubMed]
- Smith ML. Interventions to Minimize Distress During Pediatric Primary Care Visits: A Systematic Literature Review.
- Rodriguez CM, Clough V, Gowda AS, Tucker MC. Multimethod assessment of children's distress during noninvasive outpatient medical procedures: child and parent attitudes and factors. J Pediatr Psychol. 2012 Jun;37(5):557-66. [CrossRef] [PubMed]
- Daviss WB, Racusin R, Fleischer A, Mooney D, Ford JD, McHugo GJ. Acute stress disorder symptomatology during hospitalization for pediatric injury. J Am Acad Child Adolesc Psychiatry. 2000 May;39(5):569-75. [CrossRef] [PubMed]
- Lerwick JL. Minimizing pediatric healthcare-induced anxiety and trauma. World J Clin Pediatr. 2016 May 8;5(2):143-50. [CrossRef] [PubMed] [PMC free article]
- Meredith J, O′Keefe K, Galwankar S. Pediatric procedural sedation and analgesia. J Emerg Trauma Shock. 2008;1(2):88. [CrossRef] [PubMed] [PMC free article]
- American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology. 2002 Apr;96(4):1004-17. [CrossRef] [PubMed]
- Benzoni T, Cascella M. Procedural Sedation. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2024 Nov 4]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK551685/
- Godwin SA, Caro DA, Wolf SJ, Jagoda AS, Charles R, Marett BE, et al. Clinical policy: procedural sedation and analgesia in the emergency department. Ann Emerg Med. 2005 Feb;45(2):177-96. [CrossRef] [PubMed]
- Tobias JD, Leder M. Procedural sedation: A review of sedative agents, monitoring, and management of complications. Saudi Journal of Anaesthesia. 2011 Dec;5(4):395. [CrossRef] [PubMed] [PMC free article]
- Kupietzky A, Houpt MI. Midazolam: a review of its use for conscious sedation of children. Pediatr Dent. 1993;15(4):237-41.
- Rey E, Delaunay L, Pons G, Murat I, Richard MO, Saint-Maurice C, et al. Pharmacokinetics of midazolam in children: comparative study of intranasal and intravenous administration. Eur J Clin Pharmacol. 1991;41(4):355-7. [CrossRef] [PubMed]
- Bhise SB, Yadav AV, Avachat AM, Malayandi R. Bioavailability of intranasal drug delivery system. Asian Journal of Pharmaceutics (AJP) [Internet]. 2008 [cited 2024 Nov 8];2(4). Available from: http://www.asiapharmaceutics.info/index.php/ajp/article/view/203 [CrossRef]
- Acworth J, Purdie D, Clark R. Intravenous ketamine plus midazolam is superior to intranasal midazolam for emergency paediatric procedural sedation. Emergency Medicine Journal : EMJ. 2001 Jan;18(1):39. [CrossRef] [PubMed] [PMC free article]
- Practice Guidelines for Preoperative Fasting and the Use of Pharmacologic Agents to Reduce the Risk of Pulmonary Aspiration: Application to Healthy Patients Undergoing Elective Procedures: An Updated Report by the American Society of Anesthesiologists Task Force on Preoperative Fasting and the Use of Pharmacologic Agents to Reduce the Risk of Pulmonary Aspiration*. Anesthesiology. 2017 Mar 1;126(3):376-93. [CrossRef] [PubMed]
- Intranasal Midazolam [Internet]. [cited 2024 Nov 4]. Available from: https://emed.ie/Analgesia/IN_Midazolam.php
- Ramsay Sedation Scale - an overview | ScienceDirect Topics [Internet]. [cited 2024 Nov 8]. Available from: https://www.sciencedirect.com/topics/nursing-and-health-professions/ramsay-sedation-scale
- Gómez-Manzano FJ, Laredo-Aguilera JA, Cobo-Cuenca AI, Rabanales-Sotos J, Rodríguez-Cañamero S, Martín-Espinosa N, et al. Evaluation of Intranasal Midazolam for Pediatric Sedation during the Suturing of Traumatic Lacerations: A Systematic Review. Children. 2022 Apr 29;9(5):644. [CrossRef] [PubMed] [PMC free article]
- Shashikiran ND, Reddy SVV, Yavagal CM. Conscious sedation--an artist's science! An Indian experience with midazolam. J Indian Soc Pedod Prev Dent. 2006 Mar;24(1):7-14. [CrossRef] [PubMed]
- Wijdicks EFM, Bamlet WR, Maramattom BV, Manno EM, McClelland RL. Validation of a new coma scale: The FOUR score. Annals of Neurology. 2005 Oct;58(4):585-93. [CrossRef] [PubMed]
- Chiaretti A, Barone G, Rigante D, Ruggiero A, Pierri F, Barbi E, et al. Intranasal lidocaine and midazolam for procedural sedation in children. Arch Dis Child. 2011 Feb;96(2):160-3. [CrossRef] [PubMed]
- Intranasal Route - an overview | ScienceDirect Topics [Internet]. [cited 2024 Nov 4]. Available from: https://www.sciencedirect.com/topics/medicine-and-dentistry/intranasal-route
- Bellolio MF, Puls HA, Anderson JL, Gilani WI, Murad MH, Barrionuevo P, et al. Incidence of adverse events in paediatric procedural sedation in the emergency department: a systematic review and meta-analysis. BMJ Open. 2016 Jun 1;6(6):e011384. [CrossRef] [PubMed] [PMC free article]
- Singh R, Kumar N, Vajifdar H. Midazolam as a sole sedative for computed tomography imaging in pediatric patients. Paediatr Anaesth. 2009 Sep;19(9):899-904. [CrossRef] [PubMed]
- Alex S, Coelho B, Ambareesha M. Comparison of intranasal and oral midazolam as premedicant drug in preschool children. Journal of Anaesthesiology Clinical Pharmacology. 2008 Jul 1;24(3):333-6.
- Trivedi V, Doshi R, Dhuniya K. Evaluation Of Sedation Characteristics With Intranasal Midazolam Versus Sublingual Midazolam In Paediatric Patients Undergoing Magnetic Resonance Imaging. The Internet Journal of Anesthesiology [Internet]. 2009 Dec 31 [cited 2024 Nov 8];27(2). Available from: https://ispub.com/IJA/27/2/7233 [CrossRef]
- Wilton NC, Leigh J, Rosen DR, Pandit UA. Preanesthetic sedation of preschool children using intranasal midazolam. Anesthesiology. 1988 Dec;69(6):972-5. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2026.26
|
| Cite this article as: | | Kumble A, Phadke A K, Varghese A, Raikar P, Patel K, Khan S A. Comparison of Efficacy of Intravenous vs. Intranasal Midazolam for Procedural Sedation of Children Age 6 Months to 10 Years - A Single Blinded Randomized Controlled Study. Pediatr Oncall J. 2026;23. doi: 10.7199/ped.oncall.2026.26 |
|