BL Yatheesha, Ashwin Borade, L Rajam.
Department of Pediatrics, Amrita Institute of Medical Sciences, Kochi, India.
ADDRESS FOR CORRESPONDENCE
Dr.Ashwin Borade, Lecturer, Department of Pediatrics, Amrita Institute of Medical Sciences, Elamakkara Post, Edapally, Kochi-682026, Kerala, India.
Email: ashwinborade@yahoo.com | | Abstract | Objectives: To determine the prevalence of metabolic syndrome (MS) in at risk for overweight and overweight children and adolescents. Secondary objective was to estimate the distribution of the individual components of the metabolic syndrome.
Materials and Methods: For this study, a total of 81 children and adolescents at risk for overweight and overweight in the age group of 2-18 years were included in the study. Subjects were evaluated for anthropometry, waist circumference, blood pressure (BP) and biochemical parameters. Subjects who met Adult Treatment Panel (ATP) III definition modified for age were defined as metabolic syndrome.
Results: The overall prevalence of MS in the at risk for overweight and overweight children and adolescents in study was 25.9%. There was no gender difference in prevalence of MS (P=0.626). Low HDL was most common (61.7%) and hyperglycemia was the least common risk factor (2.5%). In this study the constituent factors for MS were, one factor in 27.16%, two in 35.8%, three in 21% and four in 4.9%.
Conclusion: Childhood obesity is associated with increased frequency of metabolic syndrome. We suggest screening for the metabolic syndrome should be considered in all at risk for overweight and overweight children and adolescents. | | | | Keywords | | Metabolic syndrome, cardiovascular risk factors, overweight | | | | Introduction | At risk for overweight and overweight are serious problems among young people as well as adults. The unabated rise in the prevalence of overweight in children and adolescents is one of the most alarming public health issues facing the world today. (1) The calculated global prevalence of at risk of overweight (including overweight) in children aged 5-17 years is estimated by the International Overweight Task Force (IOTF) to be approximately 10%. (2) Childhood overweight increases the risk of overweight in adulthood and is associated with cardiovascular disease (CVD) risk factors. (3,4)
The metabolic syndrome (MS) is generally defined as a cluster of cardiovascular risk factors, namely central obesity, hyperglycemia, dyslipidemia, and elevated blood pressure, which tend to aggregate in at risk of overweight or overweight individuals. (3) The criteria although similar in that they focus on overweight, dyslipidemia, hyperglycemia, and hypertension, differ in the individual constituents and threshold levels.(5)
Despite a lack of uniform definition of the syndrome in pediatrics, recent studies have shown that the syndrome develops during childhood and is highly prevalent among at risk of overweight children and adolescents. Studies in India in adult population have shown high prevalence of MS. There are only few Indian studies in children and adolescents. So this study was conducted to know the prevalence and sex difference of MS in children and adolescents and to know the distributions of various components of MS. | | | | Methods & Materials | A study was carried out in hospital from of Jan 2007 to April 2008. For the purpose of this study, at risk for overweight and overweight children in the age group between 2-18 years attending Department of Pediatrics both inpatient and out patient were enrolled in the study. A total of 81 children and adolescents with at risk for overweight and overweight were included in the study. Children who had history of primary dyslipidemia, diabetes, secondary overweight and any child receiving pharmacological treatment that could affect the metabolic profile were excluded from the study. Written informed consent was obtained from parents or guardians of all consecutive overweight patients who were enrolled for the study. The same investigator performed anthropometric measurements and complete physical examination including pubertal staging, neurological, mental and dysmorphic findings.
A complete physical examination including anthropometrics in form of height, weight, body mass index, waist circumference, hip circumference and waist to hip ratio was carried out. Height was measured in the upright position with a stadiometer. Weight was measured standing using a self-zeroing scale. Waist circumference was measured with a non-stretchable tape at the highest point of the iliac crest, in the standing position to the nearest 0.1 cm. Hip circumference was measured at the greater trochanter of the femur using a non-stretchable measuring tape. Blood pressure was measured 3-5 minute after the subject was made comfortable, using a correctly sized cuff in the right arm in the sitting position. Blood pressure was recorded twice within an interval of 5 min and the average systolic and diastolic blood pressure was taken. BP measurements were compared with reference values according to age, sex and height. Tanner classification was used for pubertal staging. Blood samples were collected after 8- 12 hours of fasting for blood glucose and lipid profile.
Subjects with BMI of more than 95th percentile on age and sex specific growth charts were classified as overweight; between 85th and 95th percentile as at risk for overweight. (4) Subjects with waist circumference at or above the 90th percentile for age and gender charts were classified as having abdominal obesity. (6) Elevated blood pressure was defined as a value at or above the 90th percentile for age, gender and height based on the updated task Force Report on the diagnosis and management of hypertension in childhood.(7) Triglyceride level more than 110mg/dl was classified as hypertriglyceridemia. (8,9) High density lipoprotein (HDL) cholesterol less than 40 mg/dl was considered abnormal. (8,9) Fasting blood glucose more than 110mg/dl was defined as fasting hyperglycemia. (8,10) Subjects who met at least three of the following five criteria; abdominal obesity, elevated blood pressure, fasting hyperglycemia, hypertriglyceridemia or low HDL were classified as having metabolic syndrome (As per Adult Treatment Panel (ATP) III definition modified for age). (8-10)
Fasting blood sugar was measured by glucose oxidase calorimetric method without deproteinization. Triglycerides estimation was done by enzymatic calorimetric test based on Wahlefed method using GPO-PAP kit in Hitachi analyzers with analytical sensitivity-detection limit: 4mg/dl. HDL-Cholesterol was estimated by homogeneous enzymatic calorimetric test based on Roche direct HDL cholesterol assay in Hitachi analyzers, analytical sensitivity-detection limit: 3mg/dl.
All the statistical analyses were performed using statistical package for social sciences (SPSS Inc., Chicago, USA) version 11.0 for Microsoft Windows. Independent t test was used to analyze the significance of difference between both groups. P value of <0.05 was regarded as significant. | | | | Results | A total of 81 children and adolescents with at risk for overweight and overweight were included in the study. Mean age was 10.6+3.16 years. Minimum age was 4 years with maximum age of 17 years. There were 12 subjects in the age-group 2 to 7 years, 35 in 7-11 years and 34 in 11-18 years. Forty-eight are males and 33 are females. Thirty-three were at risk for overweight and 48 were overweight. The overall prevalence of MS in the at risk for overweight and overweight children and adolescents was 25.9%. In the age group of 2 to 7 years, 7-11 years and 11-18 years prevalence is 16.7%, 14.3% and 41.2% respectively. The difference between the first two age groups and the last age group was statistically significant (P=0.028). There was no gender difference in prevalence of MS (P=0.626). Twenty four percent of the at risk for overweight and 27.7% of overweight group met the criteria of MS; this difference between the two groups was not significant (P=0.977). Among 34 adolescent subjects 35% of at risk for overweight and 50% of overweight adolescents met the criteria of MS. It was not significant (P=0.382). Fig. 1 shows the prevalence of various components of MS. Low HDL is more common, while hyperglycemia is the least common risk factor. Hypertriglyceridemia, central overweight, elevated BP and Low HDL are significantly associated with MS (P<0.05) as shown in Table 1.
Fig. 1 Showing the various risk factors in overweight children
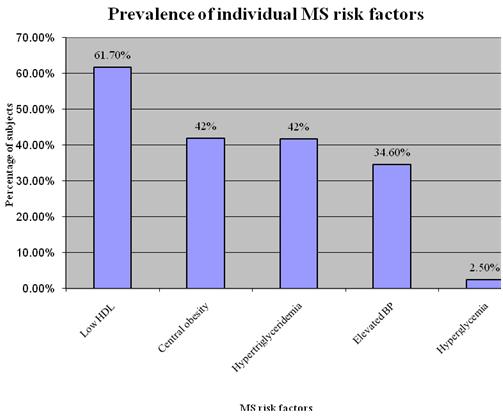
Table 1. Showing various risk factors for MS with p value
| MS risk factor |
No of Subjects |
No. of Subjects
with MS
|
P value |
| Central overweight |
Yes |
34 (41.97%) |
15 (44.1%) |
0.003 |
| No |
47 (58.02%) |
6 (12.8%) |
| Hyperglycemia |
Yes |
2 (2.46%) |
1 (50%) |
1.00 |
| No |
79 (97.53%) |
20 (25.3%) |
| Hypertriglyceridemia |
Yes |
33 (40.75%) |
18 (54.5%) |
0.0001 |
| No |
48 (59.25%) |
3 (6.3%) |
| Low HDL |
Yes |
50 (61.7%) |
20 (40.0%) |
0.01 |
| No |
31 (38.27%) |
1(3.2%) |
| Elevated BP |
Yes |
28 (34.56%) |
13 (46.4%) |
0.005 |
| No |
53 (65.43%) |
8 (15.1%) |
MS: Metabolic syndrome, HDL: high density lipoprotein, BP: blood pressure
Abdominal obesity was more common in overweight subjects and it was statistically significant (P=0.0001). Hypertriglyceridemia and elevated BP were seen more common in overweight subjects, whereas low HDL cholesterol is common in at risk of overweight subjects, but these were not significant. Hyperglycemia was seen one each in at risk for overweight and overweight individuals. In this study, the constituent factors for MS were, one factor in 27.16%, two in 35.8%, three in 21% and four in 4.9%. Eleven percent of subjects did not have any factor. | | | | Discussion | It is now emerging convincingly that MS begin in childhood (or even earlier, in fetal life), and manifest due to interactions and accumulation of various risk factors, throughout the life course. (2) MS is associated with subsequent risk of type 2 DM and CVD in adulthood. (3,4,12) The MS has not been well characterized in children and adolescents in terms of criteria, prevalence, or clinical implications. But there are studies showing the features of MS in children. (8,13) Definitions accepted for pediatric metabolic syndrome include the use of adult cutpoints or a single set of cutpoints for all ages of childhood. (14) Population-based studies of children and adolescents have used various definitions. (15) The lack of a universally accepted definition is a limiting factor in attempts to quantify present rates of metabolic syndrome. Estimates of prevalence vary considerably depending on the criteria used. (16,17)
The overall prevalence of MS in a study by Singh et al (10) in adolescents aged between 12 - 17 years from India reported 4.2%. Cook et al (8) who studied children and adolescents 12-19 years of age in the third National Health and Nutrition Examination Survey (NHANES III) data set, reported a prevalence of 4.2% and it increased to 6.4% in the NHANES study during 1999-2000. A prevalence of 3.6% was reported by investigators from the Bogalusa heart study in young adolescents of 8-17 years of age. (18) In different studies (9,19,20) the prevalence of the MS in children and adolescents aged 10-18 years ranged from 6.5% to 44.6% in overweight children and adolescents. The prevalence of MS in the present study according to the modified ATP III criteria is 25.9%. It is 24.2% in at risk of overweight group and 27.7% in overweight individuals. These observations are less than reported prevalence in other studies.
In the age group of less than 7 years, 7-11 years and 11-18 years prevalence of MS is 16.7, 14.3 and 41.2% respectively. These observations are less than Dhuper et al study (9), in the age group of less than 7 years and 7-11years. It is same as Dhuper et al (17) in the age group of more than 11 years. Ferranti et al (13) reported prevalence of 31.2% in adolescents.
Among 42% adolescents in the study group, 50% of overweight adolescent met the criteria of MS and 35% of at risk of overweight adolescent had MS. It is higher than the reported prevalence of MS in various studies. Singh et al (10) reported prevalence 36.6% in overweight adolescents and 11.5% in at risk of overweight subjects. Cook et al (8) also observed prevalence of 28.7% in overweight adolescents and 6.8% in at risk of overweight adolescents. Duncan et al (21) observed a prevalence of 32.1% in overweight adolescents and 7.1% in at risk of overweight adolescents. In a study by Serp et al reported prevalence of 2.1% in overweight children. (22)
The prevalence of the metabolic syndrome in youth may vary by sex, as it does in adults, but data on this are conflicting. In a national multiethnic study, the metabolic syndrome was significantly more prevalent in males (6.1%) than in females (2.1%), (8) but other researchers reported no significant sex differences. (10,20,23) In the present study also there is no sex difference in the prevalence of MS.
In the present study, the prevalence of low HDL, abdominal obesity hypertriglyceridemia, elevated blood pressure and hyperglycemia in adolescents are 73.5, 32.4, 50, 47.1 and 5.9%, respectively. Cook et al (8) reported low HDL, abdominal obesity, hypertriglyceridemia, elevated blood pressure and hyperglycemia in 23.3, 9.8, 23.4, 4.9 and 1.5% respectively. High prevalence of central overweight may be due to US percentile charts used in the study, as no data for waist circumference are available from India for children and adolescent population. (6) Various studies (10,13,24) also reported low HDL, hypertriglyceridemia, and central overweight as common abnormalities, whereas hyperglycemia and hypertension were infrequent abnormalities. Low HDL was the most common and hyperglycemia is the least common abnormality observed in this study, which were similar to other studies. (9,13)
The prevalence of MS in our study in subjects with low HDL, abdominal obesity, hypertriglyceridemia, elevated blood pressure and hyperglycemia was 40, 44.1, 54.5, 46.4 and 50% respectively. Hyperglycemia was present in only 2 individuals and it was not significant. In a study by Singh et al (10), the prevalence of MS in subjects with low HDL, abdominal obesity, hypertriglyceridemia, elevated blood pressure and impaired fasting glucose was 51.9, 48.8, 15.8, 38 and 11.1% respectively. In this study, MS was most common in subjects with low HDL followed by abdominal obesity. But MS was present in nearly half of those with abdominal obesity and they suggested measuring abdominal obesity as clinical marker of MS. In our study, hypertriglyceridemia was the most common abnormality associated with MS, followed by elevated BP and abdominal obesity.
In our study 88% of the subjects have one, two or more MS risk factors. Csabi et al (25) also reported 76.7% of the overweight children having one, two or more MS risk factors. In a study by Singh et al (10) one factor was most commonly present and these findings are in agreement with those of the NHANES III study data set (8) where 41% had one risk factor and the spectrum of all five risk factors was not seen in any of their subjects. In our study number of overweight subjects who had two risk factors was higher than those who had three or four risk factors indicating that at risk for overweight and overweight children and adolescents may develop MS later in life, thus predisposing them to Type 2 diabetes mellitus and cardiovascular disease.
As there is no universally accepted definition of MS in children and adolescents, it is very difficult to estimate the exact prevalence of MS. More studies including large number of sample size are required to provide the true prevalence rate of MS. | | | | Conclusion | In conclusion the overall prevalence of MS in the at risk for overweight and overweight children and adolescents is 25.9%. Hypertriglyceridemia is the commonest metabolic abnormality in subject with MS. The metabolic syndrome and its many consequences, including cardiovascular disease and type 2 diabetes will continue to increase unless we can find ways to prevent obesity and the metabolic syndrome in childhood and adolescence. The prevention and treatment of overweight in childhood should be consider a priority by pediatrician at present era.
Acknowledgement: We would like to thank all the parents and children who were part of this study.
Contributors: YBL reviewed the literature, drafted the initial manuscript and involved in data collection. AB was involved in the designing the article, revision of manuscript and will act as a guarantor for the paper. LR was involved in the involved in planning the study and in critical revision of the manuscript.
Funding- None
Competing interest- None | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Weiss R, Caprio S. The metabolic consequences of childhood obesity. Best Pract Res Clin Endocrinol Metab. 2005; 19: 405-419. [CrossRef]
- Bhave S, Bavdekar A , Otiv M. IAP National Task Force for Childhood Prevention of Adult Diseases. IAP National Task Force for Childhood Prevention of Adult Diseases: Childhood Obesity. Indian Pediatr. 2004; 41: 559-575. [PubMed]
- Goran MI, Ball GD, Cruz ML.. Obesity and risk of type 2 diabetes and cardiovascular disease in children and adolescents. J Clin Endocrinol Metab 2003; 88: 1417-1427. [CrossRef] [PubMed]
- Styne DM. Childhood and adolescent obesity. Prevalence and significance. Pediatr Clin North Am. 2001; 48: 823-854. [CrossRef]
- Cruz ML, Goran MI. The metabolic syndrome in children and adolescents. Current Diab Rep. 2004; 4: 53-62. [CrossRef]
- Fernandez JR, Redden DT, Pietrobelli A, Allison DB. Waist circumference percentiles in nationally representative samples of African-American, European-American, and Mexican-American children and adolescents. J Pediatr. 2004; 145: 439-444. [CrossRef] [PubMed]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004; 114(2 Suppl 4th Report): 555-576.
- Cook S, Weitzman M, Auinger P, Nguyen M, Dietz WH. Prevalence of a metabolic syndrome phenotype in adolescents: findings from the third National Health and Nutrition Examination Survey, 1988-1994. Arch Pediatr Adolesc Med. 2003; 157: 821-827. [CrossRef] [PubMed]
- Dhuper S, Cohen HW, Daniel J, Gumidyala P, Agarwalla V, St Victor R, Dhuper S. Utility of the modified ATP III defined metabolic syndrome and severe obesity as predictors of insulin resistance in overweight children and adolescents: a cross-sectional study. Cardiovasc Diabetol. 2007; 6: 4. [CrossRef] [PubMed]
- Singh R, Bhansali A, Sialy R, Aggarwal A. Prevalence of metabolic syndrome in adolescents from a north Indian population. Diabet Med. 2007; 24: 195-199. [CrossRef] [PubMed]
- Gogia A, Agarwal PK. Metabolic syndrome. Indian J Med Sci. 2006; 60: 72-81. [CrossRef]
- Weiss R, Dziura J, Burgert TS, Tamborlane WV, Taksali SE, Yeckel CW, et al. Obesity and the metabolic syndrome in children and adolescents. N Engl J Med. 2004; 350: 2362-2374. [CrossRef]
- de Ferranti SD, Gauvreau K, Ludwig DS, Neufeld EJ, Newburger JW, Rifai N. Prevalence of the metabolic syndrome in American adolescents: findings from the Third National Health and Nutrition Examination Survey. Circulation. 2004; 110: 2494-2497. [CrossRef] [PubMed]
- Kelishadi R. Childhood overweight, obesity, and the metabolic syndrome in developing countries. Epidemiol Rev. 2007; 29: 62-76. [CrossRef] [PubMed]
- Lambert M, Paradis G, O'Loughlin J, Delvin EE, Hanley JA, Levy E. Insulin resistance syndrome in a representative sample of children and adolescents from Quebec, Canada. Int J Obes Relat Metab Disorders. 2004; 28: 833-841. [CrossRef] [PubMed]
- Ford ES, Li C. Defining the metabolic syndrome in children and adolescents:Will the real definition please stand up? J Pediatr. 2008; 152: 160-164. [CrossRef] [PubMed]
- DeFronzo RA, Ferrannini E. Insulin resistance: a multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease. Diabetes Care. 1991; 14: 173-194. [CrossRef]
- Srinivasan SR, Myers L, Berenson GS. Predictability of childhood adiposity and insulin for developing insulin resistance syndrome (syndrome X) in young adulthood: the Bogalusa Heart Study. Diabetes. 2002; 51: 204-209. [CrossRef] [PubMed]
- Rodriguez-Moran M, Salazar-Vazquez B, Violante R, Guerrero-Romero F. Metabolic syndrome among children and adolescents aged 10-18 years. Diabetes Care. 2004; 27: 2516-2517. [CrossRef] [PubMed]
- Viner RM, Segal TY, Lichtarowicz-Krynska E, Hindmarsh P. Prevalence of the insulin resistance syndrome in obesity. Arch Dis Child. 2005; 90: 10-14. [CrossRef] [PubMed]
- Duncan GE, Li SM, Zhou XH. Prevalence and trends of a metabolic syndrome phenotype among u.s. Adolescents, 1999-2000. Diabetes Care. 2004; 27: 2438-2443. [CrossRef] [PubMed]
- Serap S, Mevlut B, Inanc C, Ender S. Metabolic syndrome in childhood obesity. Indian Pediatr. 2007; 44: 657-66. [PubMed]
- Cruz ML, Weigensberg MJ, Huang TT, Ball G, Shaibi GQ, Goran MI. The metabolic syndrome in overweight Hispanic youth and the role of insulin sensitivity. J Clin Endocrinol Metab. 2004; 89: 108-113. [CrossRef] [PubMed]
- Azizi F, Salehi P, Etemadi A, Zahedi-Asl S. Prevalence of metabolic syndrome in an urban population: Tehran Lipid and Glucose Study. Diabetes Res Clin Pract. 2003; 61: 29-3. [CrossRef]
- Csabi G, Torok K, Jeges S, Molnar D. Presence of metabolic cardiovascular syndrome in obese children. Eur J Pediatr. 2000; 159: 91-9. [CrossRef] [PubMed]
|
| Cite this article as: | | Yatheesha B, Borade A, Rajam L. Metabolic Syndrome in the at risk for overweight and overweight children and adolescents. Pediatr Oncall J. 2010;7: 100-103. |
|