Clemax Couto Sant`Anna1, Alessandra Nunes Fonseca2, Maria de Fatima B Pombo March1, Carlos Henrique Boasquevisque1, Sidnei Ferreira1, Kalil Madi1.
1Faculty of Medicine, Instituto de Puericultura e Pediatria Martagao Gesteira. Universidade Federal do Rio de Janeiro, Brazil,
2Pediatric pulmonologist, Instituto de Puericultura e Pediatria Martagao Gesteira. Universidade Federal do Rio de Janeiro, Brazil.
ADDRESS FOR CORRESPONDENCE
Dr Clemax Couto Sant` Anna, R. Cinco de Julho 350 ap. 604 - Copacabana- 22051-030, Brazil, RJ, Brazil.
Email: clemax01@yahoo.com | | Abstract | | Pulmonary carcinoid tumor is a rare malignant neoplasia in children and adolescents. The diagnosis, in general, is difficult therefore needs some degree of suspicion. We present 2 adolescents aged 12 and 15 years respectively who had recurrent pneumonia with hemoptysis. Thoracic radiography showed right perihilar and right upper lobe masses, respectively. Bronchoscopy revealed smooth surface vegetative lesions. Histopathologic findings had been characteristic of carcinoid and the follow-up was favorable in both cases. | | | | Keywords | carcinoid tumor, pulmonary carcinoid, adolescents
| | | | Introduction | | Pulmonary neoplasms are rare in children and among them, the most common is the carcinoid tumor. Wang et al (1), reviewing pediatric cases of pulmonary carcinoid tumors in the 1990's, stated that only 17 (8.1%) out of 208 patients were under 21 years of age. The mean age in children was 17 years. Until 2005, only about 35 pulmonary carcinoid tumor cases have been reported in children. (1,2) This report describes the cases of two adolescents who presented with symptoms for many months until the diagnosis was established. | | | | Case Report | Case 1
RDR, a male 15 years and 6 months of age, was referred for evaluation of a pulmonary opacity that had not responded to treatment for pneumonia and thus was investigated further. He had been asymptomatic until 14 years and 9 months of age, when he displayed repeated episodes of fever, thoracic pain in the right hemithorax, purulent expectoration and hemoptysis. Despite receiving antibiotic treatment for pneumonia, his physical examination showed no changes. Sputum smear was negative for acid fast bacilli (AFB) and the ppd was non-reactive. Thoracic radiography showed a right perihilar mass (unchanged from all previous chest x-rays) [Fig. 1]. Thoracic CT visualized a contrasting pulmonary lesion to the right, surrounding the right bronchial artery, with endobronchial involvement and extrinsic compression. Bronchoscopy revealed a smooth-surfaced vegetative lesion with regular shapes that did not compromise adjacent mucosa, located at the origin of the right lower lobar bronchus, obstructing its lumen by 95%. The lesion was brittle when touched by the bronchoscope. Endoscopic biopsy revealed neoplastic cells of regular size and shape with no evidence of mitosis and no necrotic areas. The cells formed rosette-like and ribbon patterns interspersed with a rich vascular network resulting in a diagnosis of typical pulmonary carcinoid tumor.
Figure 1: Case 1- X-ray showing right paratracheal mass

Case 2
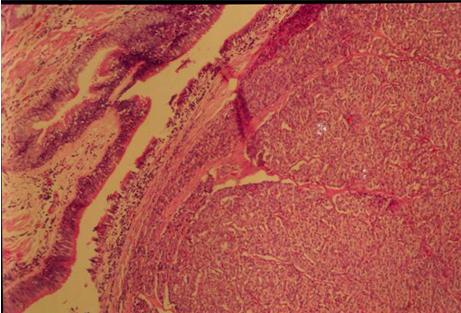
APSA, a female 12 years and 6 months of age, was referred for further investigation of a pulmonary mass in the right hemithorax that had not responded to therapy. She had been asymptomatic until 12 years and 3 months of age when she developed repeated episodes of fever, thoracic pain in right hemithorax and dyspnea at rest. Physical examination showed only decreased vesicular breath sounds in the upper two-thirds of the right hemithorax. The sputum smear was negative for AFB. Thoracic radiography showed a right apical opacity unchanged from all previous chest x-rays. A previous thoracic CT showed a mass measuring 3x2 cm with dense contrasting soft tissue, located in the superior mediastinum, occupying the right paratracheal space (Fig. 2). There was a small associated pleuropulmonary component not allowing differentiation of mass boundaries. Mediastinal lymph node biopsy revealed reactive lymphoid hyperplasia. She was diagnosed with pneumonia and treated with antibiotics. Eight months later, she had a new episode of fever, cough with purulent sputum, hemoptysis, thoracic pain and dyspnea. Thoracic radiography revealed increased opacity in the upper third of the right hemithorax. Antibiotics were given and bronchoscopy revealed a vegetative lesion at the origin of the right main-stem bronchus. Endoscopic biopsy revealed neoplasia composed of cells with a moderate amount of eosinophilic cytoplasm and small nuclei. The cells were in small groups with little connective tissue in between them (Fig. 3). The diagnosis was typical pulmonary carcinoid tumor.
Figure 2: Case 2- Mass located in the superior mediastinum occupying the right paratracheal space
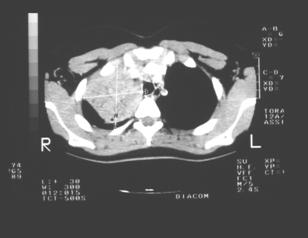
Figure 3: Case 2- Neoplasia composed of cells with a moderate amount of eosinophilic cytoplasm and small nuclei.
The endobronchial tumors of both patients were removed surgically. RDR underwent a right lower lobectomy and hilar and mediastinal lymphadenectomy. APSA underwent a right upper lobectomy, a hilar and mediastinal lymphadenectomy and a bronchoplasty after mass resection of the right primary bronchus. Histopathologic evaluation of resected specimens of both patients revealed typical pulmonary carcinoid tumor with neoplasia-free satellite lymph nodes. Both patients recovered well from the surgery and are currently asymptomatic. | | | | Discussion | Pulmonary carcinoid tumors were considered bronchial adenomas but are currently classified as malignant neuroendocrine tumors, along with small cell carcinoma and large cell carcinoma, since they are capable of synthesizing hormone-like substances similar to those produced by central nervous system (CNS) cells. (3) This neoplasia is responsible for 1 to 5% of all pulmonary tumors, without gender preference. (4) Histologic classification includes two types: typical and atypical. Typical carcinoid tumors are well differentiated, low-grade tumors, microscopically presenting less than two mitoses/mm, with no necrosis and account for approximately 90% of all cases. They are benign, are less likely to metastasize and the prognosis is good. Atypical carcinoid tumors have 2 to 10 mitoses/mm and/or coagulation necrosis. They are rarer but more aggressive, more likely to metastasize and may be related to smoking. (5) They have a worse prognosis. Histologically, our patients presented with typical carcinoid tumors involving the right main stem bronchus; this location is more common in children. (2,5-7)
Contrary to adults, children often have symptoms. They most commonly present with atelectasis, recurrent pneumonias and hemoptysis due to good vascularization of tumor. (1,2) The mean age of diagnosis in children is 17 years. The patients in both cases presented with recurring respiratory infections in the same location and hemoptysis. The interval between initial symptoms and diagnosis was one year, similar to that in literature. (1) Association with paraneoplastic syndromes due to hormonal production is rare and is related mainly to the presence of hepatic metastases. (4) Neither of our patients displayed hormone-associated symptoms.
Diagnosis is suspected when bronchoscopy shows a smooth reddened polypoid mass in the bronchial lumen. In peripheral tumors, biopsy can be transthoracic using a small needle. (4,8) Our patients were submitted to biopsy during bronchoscopy and the biopsy reports confirmed the diagnosis of neoplasia. CT revealed mediastinal and perihilar lymph nodes, justifying a more aggressive surgical resection to avoid recurrence. (6) The differential diagnosis includes tuberculosis because of the similarity between the tumor and hilar and mediastinal adenopathy. (9)
The treatment of choice is a more or less amplified surgical resection depending on the histology of the tumor, the involvement of lymph nodes, and the clinical state of the patient. Lobectomy is done in most cases (6,7,10). Cardillo et al (11) recommend that all patients undergo radical mediastinal lymphadenectomy during surgery to determine if metastases are present. Our patients underwent lobectomies with mediastinal lymphadenectomy. The lymph nodes were not affected in either patient and there were no complications during or after surgery. Adjuvant treatments such as chemotherapy and radiotherapy are not recommended for carcinoid tumors. (5) Further studies are needed to recommend the use of interferon alpha and octreotide in cases presenting metastases. (5) Prognosis varies according to the histologic type and involvement of lymph nodes. Typical tumors have an excellent prognosis and carry a 5-year survival rate of 87 to 100%. Atypical tumors have a worse prognosis and carry a 5-year survival rate of 56 to 75%. Prognosis for children is good since most pulmonary carcinoid tumors are typical and metastases are infrequent. (2,3, 7, 8,11,12). Our patients have been asymptomatic for 24 months. | | | | Acknowledgement | We thank Drs: Morgan Jackson for the revision and Luciane Alves; Monica Tura; MCM Reis, ES Ponzio and DS Brandao for their helpful cooperation.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Wang LT, Wilkins EW Jr, Bode HH. Bronchial carcinoid tumors in pediatric patients. Chest 1993; 103: 1426-1428. [CrossRef]
- Fauroux B, Aynie V, Larroquet M, Boccon-Gibod L, Ducou le Pointe H, Tamalet A, et al. Carcinoid and mucoepidermoid bronchial tumours in children. Eur J Pediatr 2005;164: 748-752. [CrossRef]
- Brambilla E, Travis WD, Colby TV, Corrin B, Shimosato Y. The new World Health Organization classification of lung tumours. Eur Respir J. 2001; 18: 1059-1068. [CrossRef]
- Fink G, Krelbaum T, Yellin A, Bendayan D, Saute M, Glazer M, Kramer MR. Pulmonary carcinoid: presentation, diagnosis, and outcome in 142 cases in Israel and review of 640 cases from the literature. Chest 2001; 119: 1647-1651. [CrossRef]
- Hage R, de la Riviere AB, Seldenrijk CA, van den Bosch JM. Update in pulmonary carcinoid tumors: a review article. Ann Surg Oncol 2003; 10: 697-704. [CrossRef]
- Mezzetti M, Raveglia F, Panigalli T, Giuliani L, Lo Giudice F, Meda S, Conforti S. Assessment of outcomes in typical and atypical carcinoids according to latest WHO classification. Ann Thorac Surg. 2003; 76: 1838-1842. [CrossRef]
- Schrevens L, Vansteenkiste J, Deneffe G, De Leyn P, Verbeken E, Vandenberghe T, Demedts M. Clinical-radiological presentation and outcome of surgically treated pulmonary carcinoid tumours: a long-term single institution experience. Lung Cancer 2004; 43: 39-45. [CrossRef]
- Rizzardi G, Bertolaccini L, Terzi A. Bronchial carcinoid tumors in children - a review. Eur Oncol Haematol 2011; 7: 196-199. [CrossRef]
- Souza GRM, Sant'Anna CC, Silva JRL, Bethlem N. Carcinoide bronquico - Relato de dois casos em criancas. J Pneumol 1984; 10: 81-84.
- Kurul IC, Topcu S, Tastepe I, Yazici U, Altinok T, Cetin G. Surgery in bronchial carcinoids: experience with 83 patients. Eur J Cardiothorac Surg 2002; 21: 883-887. [CrossRef]
- Cardillo G, Sera F, Di Martino M, Graziano P, Giunti R, Carbone L, et al. Bronchial carcinoid tumors: nodal status and long-term survival after resection. Ann Thorac Surg. 2004; 77: 1781-1785. [CrossRef]
- Abuzetun JY, Hazin R, Suker M, Silberstein P. Primary squamous cell carcinoma of the lung with bony metastasis in a 13-year old boy: case report and review of literature. J Pediatr Hematol Oncol 2008; 30: 635-637. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2012.48
|
| Cite this article as: | | Sant`Anna C C, Fonseca A N, March M d F B P, Boasquevisque C H, Ferreira S, Madi K. PULMONARY CARCINOID TUMOR AMONG ADOLESCENTS. Pediatr Oncall J. 2012;9: 70-72. doi: 10.7199/ped.oncall.2012.48 |
|