Girish Gopal, Sudha Rudrappa, Rajendra Kumar.
Department of Pediatrics, Mysore Medical College and Research Institute, Mysore, Karnataka, India.
ADDRESS FOR CORRESPONDENCE
Girish Gopal, Senior Resident, Department of Pediatrics, Mysore Medical College and Research Institute, Irwin Road, Mysore – 570001, Karnataka. India.
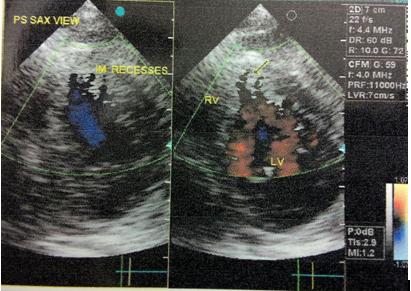
Email: girishgpl@gmail.com | | Abstract | | Isolated ventricular non-compaction (VNC) is an exceedingly rare genetic cardiomyopathy. In utero, compaction of the myocardial fibres is arrested during endomyocardial morphogenesis resulting in altered structure of the endomyocardial wall. Although this abnormality is often associated with other congenital cardiac defects, it can also be seen in isolation. Most often non-compaction of the left ventricle is seen. However, right ventricular involvement has also been reported in a few cases. Congestive cardiac failure, arrhythmias and systemic thromboembolic events are the major clinical manifestations of VNC. Two dimensional echocardiography or cardiac magnetic resonance imaging are the standard diagnostic modalities. We report a 1 ½ years old boy who presented to us with supraventricular tachycardia and congestive cardiac failure as a manifestation of isolated VNC. | | | | Keywords | | Arrhythmias, cardiomyopathy, congestive cardiac failure, echocardiography, ventricular non-compaction | | | | Introduction | | Ventricular non-compaction (VNC) is a rare genetic cardiomyopathy that is believed to arise from the arrested endomyocardial development during embryogenesis. (1) It is characterized by distinctive “spongy” morphological appearance of the ventricle and has an incidence of 0.05%. (2) Etiology of isolated VNC is not clear. However, familial cases have been reported and the mode of inheritance is heterogeneous. (3) Clinical manifestations are highly variable, ranging from no symptoms to disabling congestive cardiac failure, arrhythmias and systemic thromboemboli. Echocardiography has been the diagnostic procedure of choice, but the correct diagnosis is often missed or delayed because of the lack of knowledge about this uncommon disease and its similarity to other diseases of the myocardium and endocardium. (4) | | | | Case Report | A 1 ½ years old male child, 3rd born to 3rd degree consanguineously married couple presented to the emergency room with history of fever, cough, irritability, hurried breathing, chest in-drawing and refusal of feeds for two days prior to admission. He had 4 previous hospital admissions for pneumonia. There was no family history suggestive of heart disease. His birth history was normal without any antenatal or post natal complications. On admission, he appeared sick, irritable, had sacral edema and had significant respiratory distress (respiratory rate of 82/min) with tachycardia (heart rate of > 220/min). He was euglycemic (random blood sugar – 84mg/dl), underweight (5.5 kg) and stunted (67cms). His peripheries were cold and cyanosed with poor pulses and raised jugular venous pressure (JVP). Oxygen saturation with 8-10 litres of oxygen was around 90-95%. There were no dysmorphic features. He had a hyperdynamic precordium with a pushed down forceful apical impulse and gallop rhythm on auscultation. After the child was stabilized, a grade III pansystolic murmur was audible at the mitral and tricuspid area. Crackles were heard at the basal areas of lung fields and liver was enlarged with a span of 10 cms. There were no focal neurological deficits. An initial working diagnosis of congestive cardiac failure (CCF) with bronchopneumonia was considered. Child was managed in the pediatric intensive care unit (PICU) in a propped up position and started oxygen, ceftriaxone and amikacin, 2/3rd maintenance fluid and dobutamine infusion at 10 microgram/kg/min. Twelve lead electrocardiograph showed supraventricular tachycardia (SVT). CCF was presumed to be as a result of SVT and chemical cardioversion was done using adenosine. His heart rate and CCF improved. Chest X-ray revealed cardiomegaly with cardiothoracic ratio of 0.65 and left ventricular type of apex. Few pneumonic infiltrates were also seen in bilateral lung fields. Echocardiography showed dilated left atrium, hypertrophy of both ventricles and left ventricular ejection fraction of around 50%. Prominent trabeculations and intertrabecular recesses were found in relation to the apex, mid and apical septum, anterior wall and lateral wall of the left ventricle imparting the classic spongiform appearance (Fig 1). In addition, an equally prominent trabecular pattern and intertrabecular recesses were found involving the distal 1/3rd of the right ventricle (Fig 2). Low velocity to and fro colour flow was seen across the intertrabecular recesses in both ventricles. Trivial mitral and tricuspid regurgitation were also seen. A final diagnosis of isolated biventricular non-compaction cardiomyopathy with SVT and bronchopneumonia was made. Parents were counseled regarding the prognosis of the condition. Meanwhile, child was started on angiotensin converting enzyme (ACE) inhibitors, beta blockers and L- carnitine and discharged in a stable condition.
Figure 1: PS SAX view showing the trabeculations and IM recesses in the left ventricle.
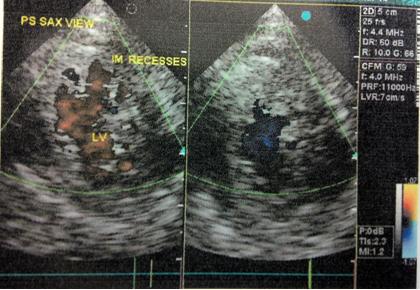
Figure 2: PS SAX view showing the trabeculations and IM recesses in the right ventricle.
 | | | | Discussion | Ventricular non-compaction (VNC) was initially described by Engberding and Bender in 1984. (5) VNC is classified by the American Heart Association as a primary genetic cardiomyopathy and is characterized by an altered myocardial wall with prominent trabeculae and deep intertrabecular recesses. (6)
Both familial and sporadic forms of non-compaction have been described. Although genes responsible for the sporadic forms have not yet been identified, genes responsible for some familial cases of VNC have been described and have been linked to a mutation in the G4.5 gene of Xq28 chromosome region. Males appear to be affected more often than females, with males accounting for 56%-82% of cases. (4,5)
VNC can occur in isolation (IVNC) or in association with other congenital heart defects. Histologically IVNC differs from VNC associated with other congenital heart diseases in that the deep intertrabecular recesses communicate with the left ventricular cavity in the former and both the coronary circulation and left ventricle in the latter. The main cause of this disorder is due to an intrauterine arrest of normal myocardial development with lack of compaction of the loose myocardial meshwork. (4) Left ventricle is uniformly affected but biventricular non-compaction has been reported, with right ventricular non-compaction described in less than one-half of these patients. Because of difficulty in distinguishing normal variants in the highly trabeculated right ventricle from the pathological non-compacted ventricle, several authors dispute the existence of right ventricular non-compaction. (4,7). Our patient had biventricular affection.
VNC can present at any age. Three major clinical manifestations of VNC are congestive cardiac failure (CCF), arrhythmias (atrial arrhythmias, ventricular tachycardia and sudden cardiac arrest) and thromboembolic events. Findings vary among patients, ranging from asymptomatic left ventricular dysfunction to severe disabling CCF. Both systolic and diastolic ventricular dysfunction has been described in these patients. (1-4)
VNC can be diagnosed by 2D and colour Doppler echocardiography. Multiple prominent ventricular trabeculations with deep intertrabecular recesses are seen. Colour doppler imaging demonstrates blood flow through these recesses in continuity with the ventricular cavity. IVNC is diagnosed when the above criteria are satisfied and coexisting cardiac lesions, such as semilunar valve obstruction and coronary artery anomalies are excluded. Although echocardiography has been the diagnostic test of choice for VNC, other modalities including contrast ventriculography, computed tomography and MRI have been used for diagnosis. MRI is particularly useful in cases with poor echocardiographic image quality. (4)
Treatment for VNC focuses on the three major clinical manifestations viz. heart failure, arrhythmias and systemic embolic events. Medical therapy with ACE inhibitors and beta blockers for systolic and diastolic dysfunction is warranted. Patients with arrhythmias may need implantable pacemakers or cardioverter-defibrillator. Prevention of embolic complications is also an important management issue, and long-term prophylactic anticoagulation has been recommended for all patients with VNC irrespective of the presence or absence of thrombus. Heart transplantation is the only option for patients with refractory CCF. (4) Since familial cases of VNC have been reported, all first degree relatives of patients with diagnosed VNC need to be screened with echocardiography in order to detect asymptomatic cases. (5)
Patients with VNC carry a uniformly poor prognosis with high mortality of upto 60% within 5 years of diagnosis. (4) Refractory CCF and ventricular arrhythmias (especially sudden cardiac death) are the usual causes of death in these patients. | | | | Conclusion | | VNC is a rare cardiomyopathy and biventricular involvement, though controversial, is even rarer. This disorder is usually accompanied by life threatening complications. Good quality echocardiography is the most important diagnostic tool. Standard medical therapy for management of CCF and arrhythmias, anticoagulants for prevention of systemic thromboembolic events play a very important role in improving the quality of life in these patients. Finally, patients with VNC should receive implantable cardioverter-defibrillator (ICD) therapy according to standard indications for primary and secondary prevention of sudden cardiac arrest. | | | | Compliance with Ethical Standards | | Funding | | None | | | | Conflict of Interest | | None | | |
- Patil VC, Patil HV. Isolated Non–compaction cardiomyopathy presented with ventricular tachycardia. Heart Views 2011; 12: 74-78. [CrossRef] [PubMed] [PMC free article]
- Awasthy N, Tomar M, Radhakrishnan S. Isolated Biventricular Non-compaction in an adult with severe pulmonary hypertension: An association reviewed. Images Pediatr Cardiol 2012; 14: 1-5. [PubMed] [PMC free article]
- Khan IA, Biddle WP, Najeed SA, Abdul-Aziz S, Mehta NJ, Salaria V. Isolated non-compaction cardiomyopathy presenting with paroxysmal supraventricular tachycardia – case report and literature review. Angiology 2003; 54: 243-250. [CrossRef] [PubMed]
- Brian C. Weiford, Vijay D. Subbarao, Kevin M. Mulhern. Non-compaction of the Ventricular Myocardium. Circulation 2004; 109: 2965-2971. [CrossRef] [PubMed]
- Srivastava A, Mahimarangaiah J, Chandrasekaran D, Manjunath. A Rare case of Biventricular non-compaction with Associated Pentad – An echocardiographic diagnosis. J Clinic Experiment Cardiol 2010; 3: 180.
- Maron BJ, Towbin JA, Thiene G. Contemporary definitions and classification of the cardiomyopathies: and American heart association scientific statement from the council on clinical cardiology, heart failure and transplantation committee; quality of case and outcomes research and functional genomics and translational biology interdisciplinary working groups; and council on epidemiology and prevention. Circulation 2006; 113: 1807-1816 [CrossRef] [PubMed]
- Ritter M, Oechslin E, Sutsch G. Isolated non-compaction of the myocardium in adults. Mayo Clin Proc 1997; 72: 26-31. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2014.33
|
| Cite this article as: | | Gopal G, Rudrappa S, Kumar R. Biventricular Non-Compaction (Spongiform) Cardiomyopathy. Pediatr Oncall J. 2014;11: 43-45. doi: 10.7199/ped.oncall.2014.33 |
|