Inês Alexandra Azevedo, Sara Sofia S. Rodrigues, Rosário Marques Da Cunha, Magalys Pereira, Virgínia Monteiro
Pediatric Department, Centro Hospitalar de Entre Douro e Vouga, Santa Maria da Feira, Portugal
Address for Correspondence: Inês Alexandra Azevedo , Avenida da Misericordia n79 4º direito, 3700-192 São João da Madeira, Portugal.
Email: Inesaazevedo1995@gmail.com
|
Question :An 8-years-old boy, previously healthy, was observed in the emergency department due to a 2-week history of edema and skin lesion in the left upper eyelid. In addition, he presented nausea, vomiting and frontal headaches with 24 hours of evolution. Fever was denied. He had previously undergone a 7-days course of treatment with topical fusidic acid and was currently on the 3rd day of oral amoxicillin + clavulanic acid 90 mg/kg/day, with no improvement. In the physical examination, the left eyelid region was erythematous with micropustules and scales, measuring 5 cm in diameter. Perilesional edema and eyelid ptosis were present, but eye movement was preserved (figure 1).
Figure 1. Initial Presentation 
The analytical study documented leukocytosis and neutrophilia. Head CT confirmed preseptal cellulitis and no changes were found in the cerebrospinal fluid.
Preseptal cellulitis associated with herpetic lesion and bacterial superinfection was assumed and the boy was admitted to the Pediatric ward for therapy with intravenous amoxicillin + clavulanic acid 150 mg/kg/day and acyclovir 30 mg/kg/day.
Due to the worsening of the edema and the skin lesions on day two of admission (figure 2), intravenous ceftriaxone 100 mg/kg/day and clindamycin 30mg/kg/day were started.
Figure 2. Day two admission. 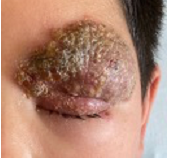
On day seven of admission (figure 3), as no signs of improvement were evident, he was evaluated by Pediatric Dermatology. The diagnosis of herpetic lesion was ruled out and the pediatric dermatology team decided to start treatment with oral griseofulvin 20 mg/kg/day for what they believed was a Kerion Celsi. Later, Candida Albicans was indeed isolated from scalp brushing.
Figure 3. Day seven admission. 
A 5-month course of oral griseofulvin was necessary for clinical cure, without complications (figure 4). The family later reported the same fungal skin lesions in the boy’s stepfather and in their two dogs.
Figure 4. Clinical cure without complications (after 5 months).  What is Kerion Celsi?
|
Discussion :
Kerion Celsi is an inflammatory form of tinea capitis and represents a delayed hypersensitivity reaction to the causative dermatophyte. The most frequent fungal agents involved are Trichophyton verrucosum, Trichophyton mentagrophytes, Microsporum canis and Microsporum gypseum.
The clinical spectrum is very variable, being more often an inflammatory well-delimited and painful plaque, with pustules and suppurative abscesses, like a “beehive” type lesion. Most cases involve the scalp and surrounding skin follicles, with an increase of regional lymph nodes.
The resulting scars can cause alopecia, so early diagnosis and appropriate therapy can prevent it.
In this clinical case, the rarity is highlighted, both by the identified agent, as well as the atypical location. | References : | - Silva SFSF, Teixeira C, Machado S, Marques L. Kérion celsi: a rare complication of tinea capitis. Revnec. 2017 Jul; 26(2):126-8.
- John AM, Schwartz RA, Janniger CK. The kerion: an angry tinea capitis. Int J Dermatol. 2018 Jan; 57(1):3-9.
- Brissos J, Gouveia C, Neves C, Varandas L. Remember kerion celsi. BMJ Case Rep. 2013
- Chiriac A, Birsan C, Mares M, Wollina U. Kerion Celsi due to Microsporum canis infection. Hautarzt. 2021 Oct;72(10):855-859.
|
|
| Correct Answers : |  100% 100% |
Last Shown : Feb 2024
|