Patient Education
The preterm/LBW infant faces several nutritional problems due to:
- Immature organ systems
- Poor suck swallow coordination till 34 weeks of gestation
- Weak suck reflex in VLBW babies
- Small gastric capacity
- Incompetent gastroesophageal sphincter, poor gag reflex
- Decreased activity of enzymes - lactases & lipases. Also decreased activity of other enzymes responsible for catabolism of tyrosine and methionine to cystine
- Decreased bile acid pool
- Low glomerular filtration rate & decreased concentrating capacity of kidney
- Smaller metabolic reserves: Decreased stores of glycogen/fat/vitamins/minerals
- Greatly increased energy requirements - due to high basal metabolic rate, increased growth, increased stress & associated metabolic problems like hypoglycemia
Feeding the baby so as to meet these greatly increased energy demands remains a nursing & nutritional art because of these special liabilities of these infants.
What Are The Nutritional Goals?
The aim of feeding should be to approximate intrauterine growth, a goal that is frequently impossible to attain. The quality of weight gained and composition of tissue accrued though difficult to measure, (protein accretion rather than fat accretion & water retention) is a better determinant of the adequacy of nutrition.
What Are the Dietary Requirements of the Various Nutrients?
The following table gives the recommendations of THE EUROPEAN SOCIETY OF PAEDIATRIC GASTROENTEROLOGY & NUTRITION (ESPGAN, 1987).
Similar recommendations have also been given by the Nutrition Committee of the American Academy of Pediatrics & the Canadian Pediatric Society.
Nutrient Requirements [ Espgan, 1987]
| Nutrient |
Requirement |
Remarks |
| Energy |
110-165 kcal/kg/day
(= 130 kcal/ kg/day) by 200 ml/kg/day of EBM
>165 a fat accretion
<110 a Inadequate |
Energy density of 65 kcal/dl (65-85 -Range) |
| Water |
150 -200 ml/kg/day
Increased in VLBW/ELBW or in conditions of insensible water losses. |
Lower intakes in height failures |
| Protein |
2.9-4.0 gm/kg/day
2.2-3.1 gm protein/100 Kcal |
* Whey predominant proteins
* Taurine content (4 mg%)
* Amino Acid content similar to breast milk |
| Fat |
4.5-9 gm /kg/day
3.6-7 gm/100 kcal |
* MCT-40% of fats
* Linoleic acid-4% of calories
* EFA -for myelinization & growth |
| Carbohydrates |
6-10 g/100 ml |
Preterm formula-50% Lactose |
| Vitamin A |
200 mcg-1000 mcg/day |
Human milk + supplemental Vitamin A |
| Vitamin D |
20-40 mcg /day |
Human milk + supplemental Vitamin D |
| Vitamin E |
0.6 mg/100 kcal |
Human milk-adequate amount. No need of supplement |
| Vitamin K |
Formula-4 mcg/100 kcal |
Breast milk + supplement 2-3 mcg/kg Vitamin K |
| Vitamin B1 |
Formula-20 mcg/100 kcal |
Breast Feeds. No supplementation required. |
| Vitamin B2 |
Formula-60 mcg/100 kcal |
Breast Feeds. No supplementation required. |
| Vitamin B3 |
Formula-800 mcg/100 kcal |
Breast Feeds. No supplementation required. |
| Vitamin B6 |
Formula-35 mcg/100 kcal |
Breast milk + supplement 35 mcg/100 Kcal |
| Biotin |
Formula-1.5 mcg/100 kcal |
Breast Feeds. No supplementation required. |
| Folic Acid |
Formula-60 mcg/100 kcal |
Breast milk + supplement 65 mcg/day |
| Vitamin B12 |
Formula-0.15 mcg/100 kcal |
No supplementation |
| Vitamin C |
Formula-7 mg/100 kcal |
Supplementation- 20 mg/day |
| Calcium |
70-140 mg/100 kcal |
Ca:P ratio of 2:1 |
| Phosphorus |
50-70 mg/100 kcal |
Breast Feeds + Supplement with 9 mg/dl |
| Magnesium |
12 mg/100 kcal |
Breast Feeds |
| Iron |
1.5 mg/100 kcal |
Breast Feeds + 2 mg/kg/day |
What are the Various Types of Feeds Available & Advantages/Disadvantages of Each One of Them?
The various types of feeds available are:
Preterm human milk
Human breast milk is considered the reference Gold standard for comparison with other kinds of milk. The various nutritional advantages (more cystine & taurine, better fat absorption; greater bioavailability of trace elements like Iron), as well as non-nutritional advantages of human milk (immunological & antimicrobial protection, hormones & growth factors, emotional, etc), are well established. These are of special importance to LBW babies with immature gut & susceptibility to infections.
It is amazing that the composition of preterm mother's milk is suited to the increased requirements of certain nutrients of the preterm baby.
Thus, milk of mother delivering prematurely has a higher content of proteins, sodium, fatty acids, energy, Ca+, Mg+, Zn, Cu, Fe, IgA & other host defense factors. These differences are more marked between 28 - 32 weeks of gestation.
Gastric emptying is faster with human milk than formula milk.
Many studies comparing long term neurodevelopment outcomes have shown higher scores on babies fed human milk.
Thus, preterm milk if fed at higher volumes of 180-200 ml/kg/day may provide adequate calories & proteins in most LBW babies (especially in babies weighing 1.5 - 2.5 kg) & is the ideal feed.
However, there are practical problems:
- The mother may not be available in the NICU.
- The rates of secondary lactation failure are high in these mothers who are emotionally stressed & worried due to multiple factors like separation of babies who are kept in NICU, sick babies, etc.
Thus, one has to consider other alternatives. Also in VLBW babies, human milk may not meet the increased nutritional demands.
Bank human milk
There are various disadvantages of using milk from breast milk banks. Heat treatment (which is essential to prevent the spread of infection) & storage destroys the important anti-infective factors (IgA, IgG, lactoferrin, etc). Also, since most of the banked milk is derived from full-term donor mother's drip milk (drip milk has very low calories & protein content), it is likely to be inadequate for the LBW baby's need.
Animal (cow's) milk
Fresh dairy milk is an easily available & affordable breast milk substitute, which is traditionally used in our country. It can be humanized by diluting it & adding sugar. Thus, it could match the protein & energy content of breast milk quantitatively but there are definite qualitative differences in the various components, which are not suited for the optional growth of LBW baby. The disadvantages are:
- High solute load due to excess sodium & proteins, which the immature kidneys cannot handle.
- Different whey:casein ratio (80:20)
- Allergenic properties (more important in the family history of atopy)
- Poor in essential fatty acids, iron & minerals.
AAP has recommended against the use of dairy milk in 1st 6 months of life. This is obviously impractical in our country where cow's milk forms a cheaper alternative to breast milk. The other advantage is that no preparation (as opposed to formula milk) is required thereby reducing the chances of infection.
Formula milk
These are artificially prepared to match the breast milk composition of various nutrients & are considered the next best alternative to breast milk. They are based on various recommendations given by committees on the nutrition of LBW.
Regarding the use of formula milk, it is extremely important to have correct handling of these formulae as unhygienic preparation & wrong dilution can prove extremely hazardous to the baby.
Therefore, the formula should be used only if one is convinced that the mother can afford it & can use it hygienically & incorrectly dilution.
What are the Types of Fortifiers?
What are the Various Techniques of Feeding & Guidelines for Using Them?
There are various techniques for feeding an LBW baby. They are:
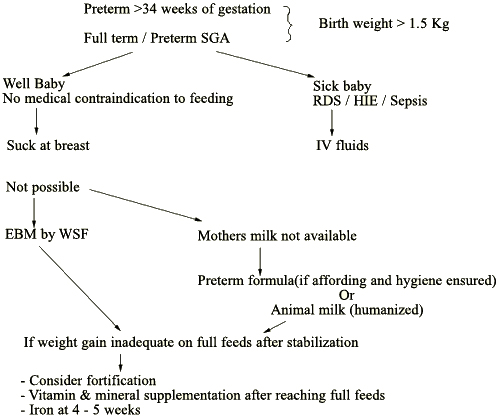
- Breast Feeding: Done in larger preterms (>1.5 kg and >34 weeks of gestation) and full term LBW babies.
- Oral feeds by Wati and spoon: Used in VLBW babies who have a weak suck or have significant energy expenditure in sucking (as evidenced by poor weight gain) after ruling out other causes of weak suck and poor weight gain.
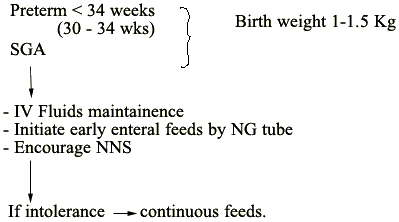
- Nasogastric feeds: Used to initiate feeding in babies less than 34 weeks of gestation. Also in all babies who are improving from sepsis/asphyxia or any other neonatal conditions.
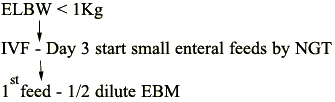
- Continuous nasogastric/transpyloric feeds: Used in ELBW babies.
- Non-Nutritional Sucking
Guidelines for Feeding
Monitor
| For tolerance |
For nutritional status |
| - RT aspirate |
- Daily weight |
| - Abdominal girth |
- Hb/HC/skin fold thickness- weekly
|
| - Stool for occult blood |
- S. albumin/Ca/Phos/Alk. Phos/VBG-once in 2 weeks -
|
- If poor weight gain: inadequate calories/proteins
- Increased BUN/metabolic acidosis: excessive protein intake
- Poor growth/low BUN/low albumin: inadequate protein intake
- Increased triglyceride levels: fat intolerance
Abbreviations
| EBM= Expressed breast milk |
Hb= Hemoglobin |
| WSF= Wati spoon feeds |
HC= Head Circumference |
| RDS= Respiratory Distress Syndrome |
S. albumin= Serum albumin |
| HIE= Hypoxic Ischemic Encephalopathy |
Ca= calcium |
| NG= Nasogastric |
Phos= Phosphorus |
| NNS= Non nutritive sucking |
Alk. Phos= Alkaline Phosphate |
| IVF= Intravenous Fluids |
VBG= Venous blood gas |
| NGT= Nasogastric tube |
BUN= Blood urea Nitrogen. |
| RT= Ryle's tube |
|