A case of Clostridioides difficile infection in an infant with COVID-19: A reminder of judicious antibiotic use
Ana Rita Barroca de Macedo1, Beatriz Vilela de Carvalho Taveira Pinto1, Catarina Maria Queirós Fraga1, Sofia Carolina Costa Jordão2, Rui Manuel Correia de Almeida1
1Department of Pediatrics, Hospital Pedro Hispano, Matosinhos, Portugal, 2Department of Infectious Diseases, Hospital Pedro Hispano, Matosinhos, Portugal
Address for Correspondence: Ana Rita Barroca de Macedo, Rua Eduardo Torres, 4464-513 Senhora da Hora, Matosinhos, Portugal.
Email: ritabarrocamacedo@gmail.com
Keywords: Clostridioides difficile, COVID-19, C. difficile toxin, Stool enzyme immunoassay, Vancomycin
Clinical Problem :
A previously healthy seven-month-old female infant presented to the paediatric emergency department with a three-day history of high fever, persistent cough, and increased work of breathing. On physical examination, she had polypnea (respiratory rate of 80/min), with pronounced chest wall retractions, and bilateral crackles on auscultation, prominent at the right lung base. A nasopharyngeal swab tested positive for SARS-CoV-2 via polymerase chain reaction (PCR).
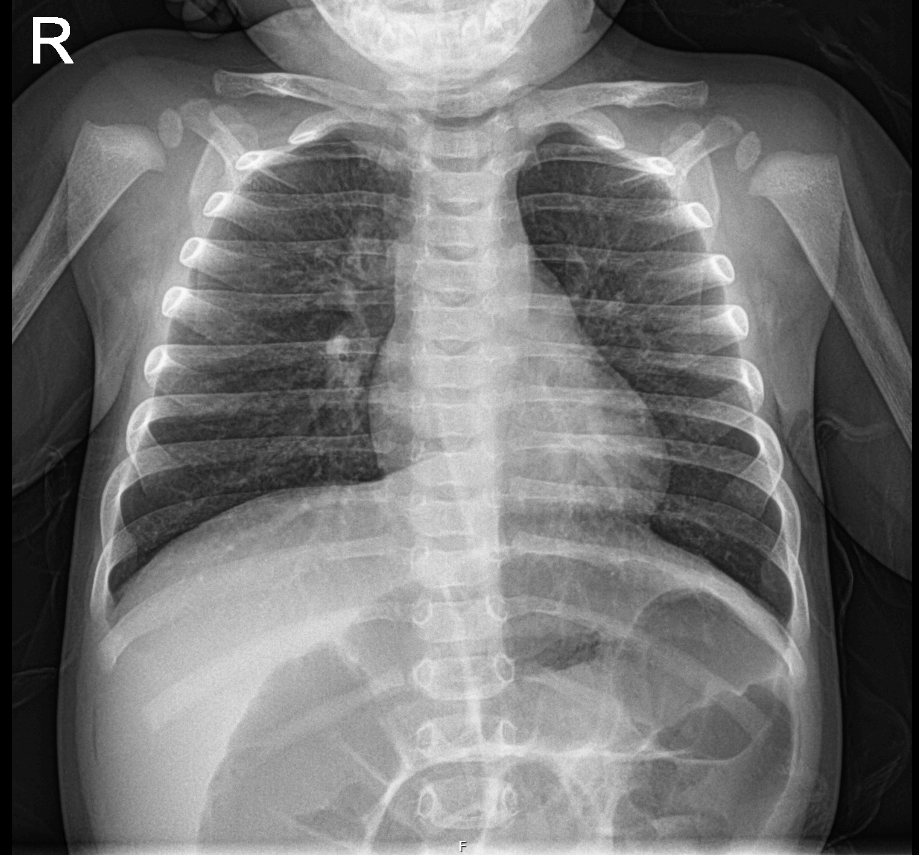
Initial blood tests showed an isolated elevation of C-reactive protein (CRP) to 286 mg/L. Chest radiography revealed bilateral peribronchial markings and decreased transparency in the right pericardiac region, suggestive of COVID-19 pneumonia with possible bacterial superinfection (Figure 1). Intravenous Ampicillin (200 mg/kg/day every 6 hours) was initiated, and the patient admitted in our Paediatric facility.
During hospitalization, the infant developed hypoxia, prompting evaluation by the infectious diseases team. Treatment with intravenous remdesivir and Dexamethasone was started per hospital protocol, for five days. Even though respiratory symptoms were resolved by the end of antiviral treatment, patient remained uncomfortable, with increasing food aversion and developed watery and profuse diarrhoea, with over 10 stools per day, without visible blood or mucus, despite feeding modifications and probiotic therapy. On the 9th day of hospitalization, the patient experienced sudden clinical deterioration: hypotension (60/30 mmHg), tachycardia, sunken eyes and fontanelle, dry mucous membranes, and lower abdominal tenderness. A 7% weight loss was documented. Laboratory workup revealed hyponatremia (Na? 129 mmol/L), hypokalemia (K? 2.9 mmol/L), leukocytosis (28,000/µL) with neutrophilia, and CRP of 16.1 mg/L. Renal function remained normal. She received fluid resuscitation with isotonic crystalloid (20 mL/kg) and maintenance therapy. Stool enzyme immunoassay (EIA) was positive for Clostridioides difficile (C.difficile) toxins A and B. Ampicillin was discontinued, and oral Vancomycin (40 mg/kg/day divided every 6 hours) was initiated.
Within 48 hours, the patient showed marked improvement, with reduced stool frequency, improved appetite, and better overall appearance. She was discharged on hospital day 15 to complete a 10-day course of oral vancomycin.
Figure 1. Chest radiography at the emergency department showing bilateral peribronchial markings with decreased transparency in the right pericardiac region.
|
In infants hospitalized with viral respiratory infections such as COVID-19, how can clinicians prevent and manage Clostridioides difficile infection effectively?
Discussion :
There is scarce available data regarding COVID-19 in infants and symptomatic infection with C. difficile.
The clinical spectrum of COVID-19 in children ranges from asymptomatic to life-threatening disease, though the majority present with mild or no symptoms. Clinical features often overlap with those of other viral illnesses, such as bronchiolitis and gastroenteritis. 1 Unlike other respiratory viruses such as influenza, SARS-CoV-2 is infrequently associated with secondary bacterial infections. SARS-CoV-2 infection frequently provokes a systemic inflammatory response, which may lead to elevated inflammatory markers. 2 Misinterpretation of these findings can result in unnecessary and prolonged antibiotic use. This approach carries risks, especially in infants, where exposure to broad-spectrum antibiotics - particularly beta-lactams - has been associated with disruption of gut microbiota and increased risk of C. difficile infection.
C. difficile is a leading cause of antibiotic-associated diarrhea. Although colonization with toxigenic strains is common in infants, progression to symptomatic infection is less frequent. When it does occur, it may range from mild diarrhea to severe colitis. 3 Recent epidemiologic trends show a rising incidence in the pediatric population, sometimes requiring intensive care or prolonged hospitalization.
Diagnosing C. difficile infection in infants is challenging due to the lack of validated criteria for assessing severity and the inability of current stool tests to distinguish colonization from infection. 4 Therefore, testing should be reserved for symptomatic cases with systemic signs, particularly when risk factors such as recent antibiotic exposure are present. The cornerstone of treatment includes prompt discontinuation of the inciting antibiotic and initiation of targeted therapy. 5 In this case, Vancomycin was effective. Supportive care with fluid and electrolyte management is also essential.
This case underscores the importance of antimicrobial stewardship in pediatric care. Misinterpretation of laboratory and imaging findings in viral infections may lead to avoidable antibiotic prescriptions, which in turn can result in serious complications such as C. difficile infection. Clinicians should exercise caution in initiating empiric antibiotics in infants with suspected COVID-19, reserving them for cases with strong evidence of bacterial co-infection. | References : | - Minciu, M., Leica, I., Balasa, A., Frecus, C., L, M., Pantazi, A. C., Cuzic, V., Chisnoiu, T., & Mihai, C. M. (2022). Clinical and Evolutionary Features of SARS-CoV-2 Infection in Children. ARS Medica Tomitana. https://doi.org/10.2478/arsm-2022-0038
- Sayegh, M. N., Cooney, K. A., Wang, L., Hoang, T., Viox, E. G., Pino, M., Schneider, F., Geller, R., Paiardini, M., & Levit, R. D. (2020). Systemic Inflammation in Acute SARS-CoV-2 Infection May Lead to Elevated Cardiac Cytokines and Adverse Remodeling. Circulation Research, 127(12). https://search.bvsalud.org/global-literature-on-novel-coronavirus-2019-ncov/resource/es/covidwho-1186419
- Shirley, D.-A., Tornel, W., Warren, C. A., & Moonah, S. (2023). Clostridioides difficile Infection in Children: Recent Updates on Epidemiology, Diagnosis, Therapy. Pediatrics. https://doi.org/10.1542/peds.2023-062307
- Watkin, S., Yongblah, F., Burton, J. R., Hartley, J. C., & Cloutman-Green, E. (2024). Clostridioides difficile detection and infection in children: are they just small adults? Journal of Medical Microbiology, 73(3). https://doi.org/10.1099/jmm.0.001816
- Cymbal, M., & others. (2024). Management of Clostridioides difficile infection: Diagnosis, treatment, and future perspectives. The American Journal of Medicine, 137(7), 571-576. https://doi.org/10.1016/j.amjmed.2024.03.017
|
| Correct Answers : |  0% 0% |
|
|
|
|
|
|