Congenital Hydrocephalus: Communicating or Obstructive_?
Jogender Kumar, Amitabh Singh
Department of Pediatrics, All India Institute of Medical Sciences, New Delhi, India
Address for Correspondence: Dr. Jogender Kumar` Senior Resident, Pediatrics, Post Graduate Institute of Medical Education and Research, Chandigarh, India.160012.
Email: jogendrayadv@gmail.com
Clinical Problem :
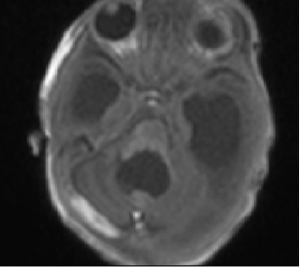
A two-month-old boy presented with irritability, recurrent episodes of projectile vomiting for 3 days and rapidly increasing head size for 15 days. There was no fever. He was born at term and had a birth weight of 2.69 kg with uneventful perinatal course. Baby was on breast feeds. On examination, anterior fontanelle was tense and bulging and there were widely separated squamoparietal sutures. He had sun setting of the eyes. Lumbar puncture was tried three times by different pediatricians but every time, it was a dry tap. On ventricular tap, 30 ml of cerebrospinal fluid {CSF} was removed following which irritability improved. A bedside cranial ultrasound {Figure 1} showed dilated lateral, third and fourth ventricles suggestive of communicating hydrocephalus. MRI brain {Figure 2} also showed all four ventricles dilated suggestive of communicating hydrocephalus.
Figure 1. Ultrasound of the skull shows dilated lateral, third and 4th ventricles
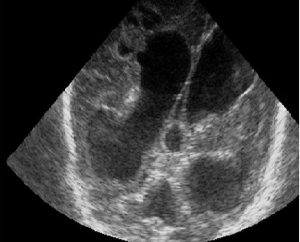
Figure 2. MRI shows all 4 ventricles dilated
|
Is it is really communicating hydrocephalus_? If yes, then why was the lumbar puncture a dry tap_?
Discussion :
For such a large communicating hydrocephalus` if the obstruction is at subarachnoid granulations then there must be CSF filled subarachnoid space. However, there is no fluid in the subarachnoid space. The only possibility is there is no CSF beyond the fourth ventricle which can explain the dry lumbar tap. In view of above picture, possibility of obstruction at the level of the foramen of Magendie and Luschka was kept. The baby was taken for surgery in view of worsening hydrocephalus. During surgery, a dye was put in CSF and it was found that there was no dye going beyond the fourth ventricle so a diagnosis of atresia of foramina of Magendie and Luschka was considered. Atresia of the foramina of Magendie and Luschka is a rare cause of obstructive hydrocephalus` in literature only few cases are described. {1} As clinical features are like Dandy Walker malformation` so some authors consider it as a spectrum of the same. As seen in our patient, this entity presents as communicating hydrocephalus. Magnetic resonance imaging in such cases shows slight dilation of all the ventricles along with a significantly dilated fourth ventricle. In absence of aqueductal stenosis the enlargement of both lateral recesses of the fourth ventricle suggests the possibility of an atresia of the foramina of Magendie and Luschka. {2} The classical treatment for this entity was CSF shunting. However, recent treatment includes endoscopic ventriculostomy. Giannetti et al successfully treated one case of atresia of foramina of Magendie and Luschka by fourth ventriculostomy. {2} In our patient ventriculoperitoneal shunt was done in view of high pressure hydrocephalus.
Almost all of congenital hydrocephalus are communicating {3} but this special entity causes obstructive hydrocephalus which radiologically mimics as communicating. In such cases lumbar tap should be avoided as it may lead to herniation of brain stem. | References : | - Maloney AF. Two cases of congenital atresia of the foramina of Magendie and Luschka. J Neurol Neurosurg Psychiatry. 1954;17:134-138.
- Giannetti AV, Malheiros JA, da Silva MC. Fourth ventriculostomy: an alternative treatment for hydrocephalus due to atresia of the Magendie and Luschka foramina. J Neurosurg Pediatr. 2011; 7:152-156.
- Volpe JJ. Neurological Proliferation, Migration. Organization and Myelination. In: Neurology of the Newborn. Vol 899. 5th edn. Saunders. Philadelphia. 2008: 93
|
| Correct Answers : |  15% 15% |
|
|
|
|
|
|