João Pedro Faria Dias, Ana Catarina Soares Feio de Azevedo, Clara Isabel Bessa Vieira, Hernâni Fernando da Costa Brito.
Pediatrics Department, Centro Hospitalar do Médio Ave, Vila Nova de Famalicão, Portugal.
ADDRESS FOR CORRESPONDENCE
João Pedro Faria Dias, Rua António Costa Pereira, nº25 Hab 504, São Mamede Infesta, Matosinhos, Portugal.
Email: fariadias94@gmail.com | | Abstract | | Pityriasis rosea (PR) is a common, self-limited skin disease that primarily affects children and adolescents. It is characterized by the appearance of an oval-shaped, scaly rash that typically begins with a single patch known as the herald patch. The exact cause of this condition is not known, but it is believed to be related to viral infections. The diagnosis is based on history and physical examination of the rash and this entity should be distinguished from several diseases, including secondary syphilis. This article reports three PR cases in children and reviews the etiology, clinical features, differential diagnosis and management of PR in pediatric patients. | | | | Keywords | | Pityriasis rosea, Childhood exanthems, Case reports. | | | | Introduction | Pityriasis Rosea (PR) is a frequent and acute skin condition that was initially dubbed exanthema pityriasis rosea by Gilbert in 1860 and first reported by British physician Rober Willan in 1978.1 This illness often begins with a "herald patch" on the trunk and progresses to a self-limited papulosquamous eruption over the trunk and proximal regions of the limbs. Seventy-five percent of all cases are documented between the age range of 10 to 35 years old, which is when it often occurs.2 Affecting youngsters under the age of ten is rare.2 Although the distribution of sexes appears to be uneven, some research indicates that females are more frequently impacted.3,4 It happens consistently all year long with no statistically significant variations.5
Although the exact cause of this illness is yet unknown, infectious organisms, drugs and environmental factors are the primary contributing causes.6
A thorough history taking and physical examination are the foundations for the diagnosis of PR. The differential diagnosis should take into account a number of disorders, including drug eruption, lichen planus, psoriasis, dermatophytosis, secondary syphilis and atopic dermatitis. UV light B phototherapy, topical emollients, oral antihistamines and corticosteroids are the mainstays of the treatment.7
This article's current goal is to present a literature review and case report of Pityriasis Rosea in children, which can assist with the condition's diagnosis, causation and treatment. | | | | Case Report | Case 1
A 15-year-old female adolescent presented with pruritic skin eruptions, with two weeks of evolution, located on the trunk, face and extremities. The first lesion, the “herald patch” was noted on the left thigh. Most of the lesions were oval and aligned themselves along the body lines of cleavage (Figure 1). The patient had an upper respiratory tract infection in the week prior to the onset of the lesions. She was treated with oral antihistamines (hydroxyzine), topical hydrocortisone for larger lesions and emollient cream. As the symptoms persisted after four weeks and due to maternal anxiety, she was evaluated by dermatology and treated with a course of prednisolone. The symptoms resolved after eight weeks without any sequelae.
Figure 1. Multiple erythematous, scaly papules and plaques in a "Christmas tree" pattern on the back.

Case 2
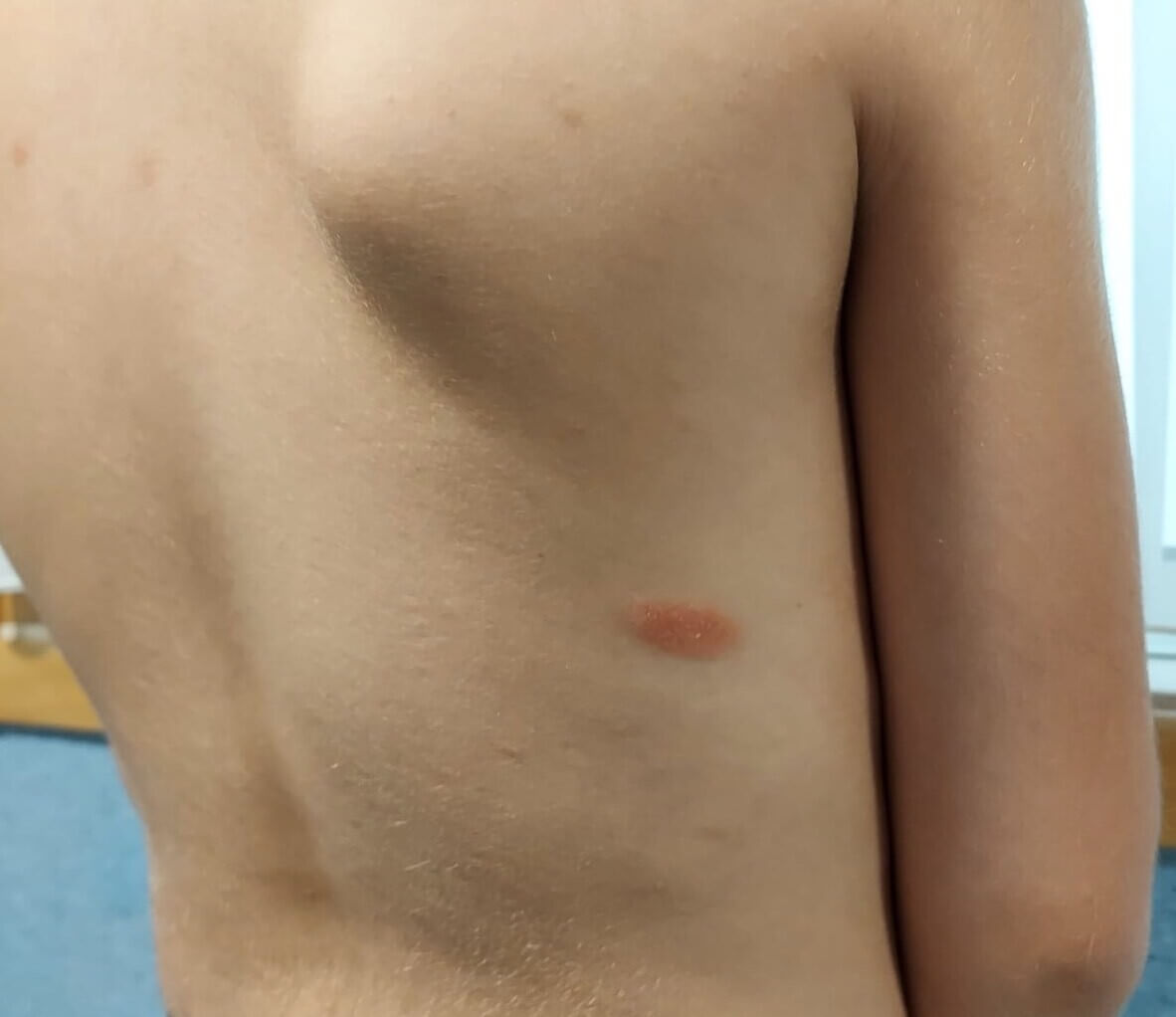
A 7-year-old boy, with a past medical history of asthma, was evaluated for pruritic skin lesions that have been present for seven days on the trunk area and had progressed to the limbs. The first lesion appeared on the right dorsal region (Figure 2). He had a history of a viral respiratory infection in the two weeks prior to the onset of the condition. The patient was treated with oral antihistamines, topical corticosteroids and emollients. After 3 weeks, the rash was completely resolved without any sequelae.
Figure 2. Some erythematous papules on the trunk and an erythematous herald patch with slightly elevated scaling borders on the right midback.
Case 3
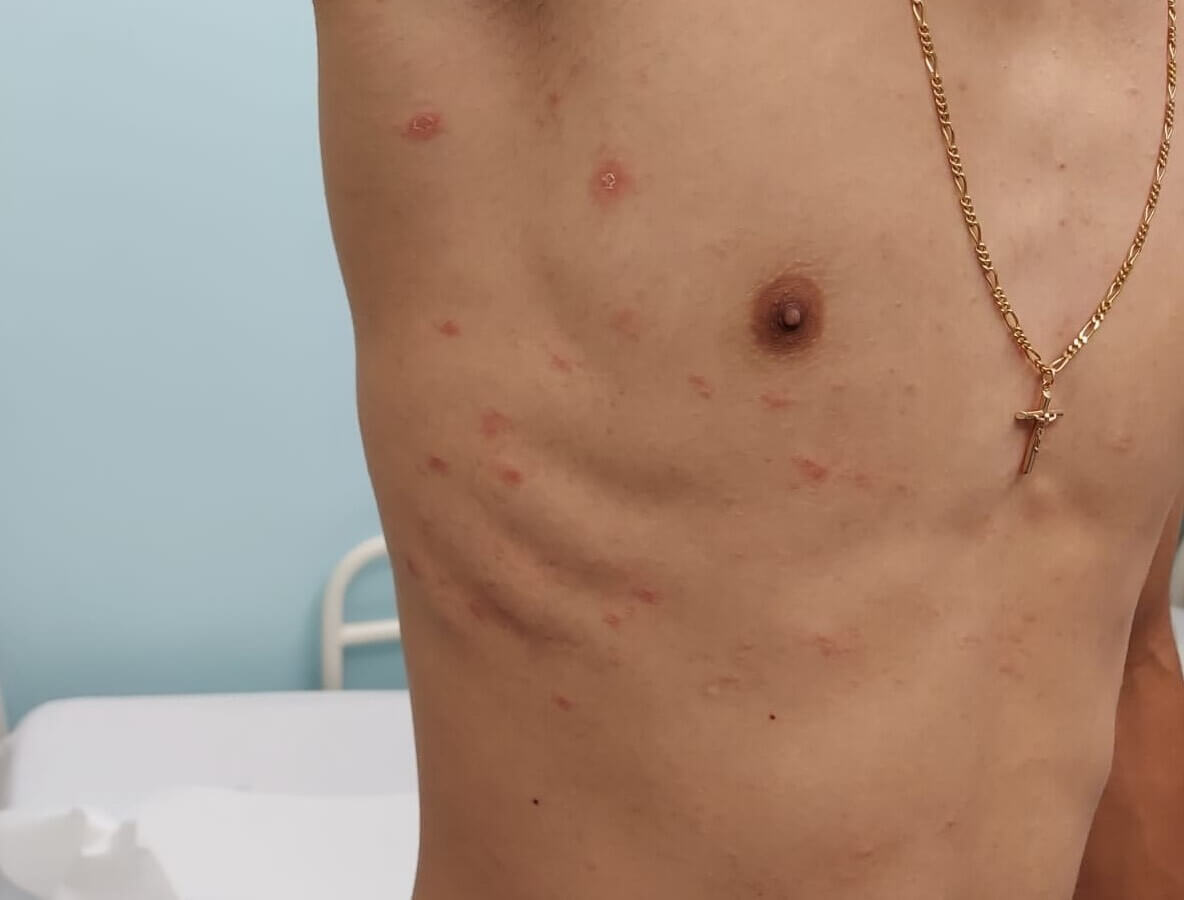
A previously healthy 17-year-old boy was evaluated for a seven-day history of an itchy rash (Figure 3). A distinct herald patch was noted on the trunk and the lesions progressed to the limbs. He had flu-like symptoms in the week before the onset of the lesions and had tested negative for SARS-CoV-2. He was treated with oral antihistamines, topical corticosteroids and emollient cream. The lesions resolved within 6 weeks.
Figure 3. Typical pityriasis rosea rash on the chest with multiple round or oval erythematous plaques with fine scaling with associated herald patch.
ETIOLOGY
Numerous observations support the theory that pityriasis rosea has a viral etiology: There are times when fever, headache, malaise and pharyngitis precede or accompany PR. It can show up in tiny case clusters at times and no correlation between bacterial or fungal species and it has been seen.6,8,9 The increase in CD4 lymphocytes and Langerhans cells in dermis also corroborated the viral etiology.10
Human herpesviruses 6 and 7 have been identified by recent investigations (HHV-6 and -7). The two viruses most frequently linked to PR are HHV-6 and HHV-7. Interactions between these viruses may account for recurrences and unusual appearances.11,12
This disorder may be brought on by the cutaneous infiltration of latently infected lymphocytes during systemic viral replication rather than by a direct herpesviral infection within the skin.8,9
But given the limited and inconsistent nature of the studies connecting HHV-6 and -7 to PR, further research is required to fully comprehend the pathophysiology of this illness.9 The H1N1 influenza A virus and human herpesvirus 8 are two more viruses that have been linked.6,13
CLINICAL PRESENTATION
PR usually starts as a single oval, scaly, erythematous plaque (sometimes called a "herald patch") on the neck or trunk that is between two and five centimeters in size. Because a herald patch is asymptomatic, especially if it is on the back or flank, some patients may not experience a herald patch before developing a broad rash or may not even recall having one.8,9 In a matter of one to two weeks, the trunk, the proximal regions of the extremities and the lines of skin cleavage that produce the distinctive "christmas tree" pattern all see the development of numerous smaller papulosquamous lesions.6,8,9 Although these lesions resemble the herald patch, they have a more pink tint.14
It is possible to identify several unusual forms of PR, especially in younger individuals. In certain situations, an inverted pityriasis rosea may develop, with the rash primarily affecting the face and distal extremities and/or the pubic, inguinal and axillary regions.6,8,15 Black children typically have an inverted pattern, affecting the face (30%) and scalp (8%) with the majority still having persistent pigmentary abnormalities.4,16 PR unilateral, lichenoid vesicular, papular, purpuric, erythema multiforme-like and urticarial forms are some more unusual appearances.17
Although they are typically asymptomatic, oral mucosal lesions such as punctate hemorrhages, ulcerations, erythematous macules and vesicles may also be involved.8,18
Although pruritus is a rather frequent complaint, in certain circumstances it can be severe or asymptomatic.8,9 PR often has negligible effects on children's quality of life.4
Prodromal symptoms such as fever, arthralgias, headache, stomach discomfort and malaise precede about 5% of clinically typical cases of PR.9,13
Longer and shorter periods of pityriasis rosea have been documented, but the average course lasts two weeks to several months.4,9 Recurrence rates have been reported to range from 1.8 to 3.7%.13,19
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of pityriasis rosea includes several conditions (Table 1). If the diagnosis is uncertain, a skin biopsy can be performed to exclude other pathologies.6,9
Table 1. Differential diagnosis of Pityriasis Rosea.
| Condition |
Distinguishing characteristics |
| Secondary Syphilis |
Involvement of the palms and soles with red-brown macules and does not begin with a herald patch. Generalized lymphadenopathy with evidence of a primary chancre. A VDRL (venereal disease research laboratory) should be considered in any patient with PR, especially in adolescents when secondary syphilis is suspected. Atypical lesions or no herald patch ? Serologic tests for syphilis (RPR - rapid plasma reagin/VDRL and treponemal antibody test) are recommended. |
| Tinea Corporis and Tinea versicolor |
Lesions with borders that may be papular, pustular, scaly or vesicular. The active border should demonstrate hyphae on cytological examination or culture positive. Tinea versicolor can be distinguished by its distribution (upper trunk, neck and face), color (hyperpigmented or hypopigmented rather than erythematous) and the presence of finer scale than in PR. The diagnosis can be made by detecting hyphae and spores on a KOH mount of infected scales or by use of a Wood’s light. |
| Guttate Psoriasis |
A form of psoriasis often seen in children following a streptococcal infection. Presented by round and ovoid scaly, erythematous macules on the trunk. It can be differentiated by history (lack of herald patch) and by exam, as the psoriasis macules have a thicker scale. |
| Nummular Eczema |
Presents with intensely pruritic, single or several “coin-shaped” lesions, usually confined to the back of the hands. It should rapidly improve with topical steroids and emollients. Serous exudate may be present in acute lesions. A biopsy demonstrates spongiosis in the epidermis. |
| Pityriasis lichenoide chronica |
An uncommon condition that is characterized by recurrent crops of erythematous to brown scaly papules on the trunk and proximal extremities. Usually, it does not begin with a herald patch. The disorder may persist for months or years before full resolution. |
| Cutaneous Lupus |
One subtype - subacute cutaneous lupus erythematosus (SCLE) has a similar appearance to PR. It can be distinguished from PR primarily because it doesn't tend to affect covered areas such as the lower chest and back. Biopsy and Anti-SS-A/Ro and anti-SS-B/La autoantibodies allow the diagnosis. |
| Pityriasis rosea-like drug eruption |
Frequently lack a herald patch, oral lesions and postinflammatory hyperpigmentation are more common. Drugs that can produce PR-like include barbiturates, bismuth, captopril, clonidine, metronidazole, sulfasalazine, gold, imatinib mesylate, interferon, omeprazole, terbinafine, isotretinoin and lithium. It can also occur after influenza, H1N1, diphtheria, smallpox, hepatitis B, pneumococcus and coronavirus disease 2019 vaccination. |
Information from references 6,8,9,13,14,20.
Other disorders that should be considered in the differential diagnosis of PR include Lyme disease, human immunodeficiency virus (HIV) seroconversion illness and viral exanthems.
TREATMENT
Pityriasis rosea has a self-limited course that permits a watchful waiting strategy in which most patients can be managed with just education, reassurance and pruritus therapy.6 To comfort patients and caregivers, it is crucial to convey information about the clinical course, infectivity and relapse. It should be clarified that the rash is benign and non-contagious and usually goes away on its own in two to twelve weeks. Additionally, they should be reassured that skipping school or other activities is not necessary.6,8,9
Oral antihistamines, topical corticosteroids (medium potency) and emollients (including menthol or pramoxine) can all help reduce itching.6,8 For two to three weeks, pruritic areas can be treated with topical steroids two or three times a day.6
UVB phototherapy should be taken into consideration in severe cases where the patient's quality of life is significantly negatively impacted by the disease and it is widespread. While PR can be made less severe with this treatment, the course of the disease and pruritus are unaffected.9,10
At the moment, medications like ganciclovir and acyclovir don't seem to work well in kids.8,9
Acyclovir has been demonstrated in adult research to be beneficial in lowering symptoms; however, because of the lower frequency of systemic symptoms and average severity of rash, its treatment is not advised in pediatric instances.21 For PR, the effectiveness of macrolides such as clarithromycin, azithromycin and erythromycin is unclear and does not seem to be very effective.6
Pediatricians or primary care providers can typically handle most situations. If the rash lasts longer than three months, the symptoms are severe, or the diagnosis is unclear, a dermatology clinic referral might be required.12
| | | | Conclusion | Pityriasis rosea is a skin condition that typically affects school-age children and rarely occurs in children under the age of ten. Only one patient in our recorded cases was younger than this, but the disease progressed normally in most of the other cases.
According to the literature, the disease typically manifests as a herald patch at first, which is followed by a rash that spreads over the trunk and the closest parts of the limbs and has oval lesions that are comparable in size. The instances that were reported further corroborated the existence of a viral infection prodrome, as documented in the literature. The recommended course of treatment for PR is symptomatic treatment and there is extremely little chance of recurrence.
This review aims to emphasize the importance of recognizing this clinical entity and clarifying the diagnosis, where the clinical history and physical examination play crucial roles in its definition, thereby avoiding unnecessary investigations and treatments. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Percival GH. Pityriasis rosea. Br J Dermatol Syph 1932; 44:241 - 253. [CrossRef]
- Youngquist S, Usatine R: It's beginning to look a lot like Christmas. West J Med. 2001, 175:227-228. [CrossRef] [PubMed] [PMC free article]
- Chuh AA, Dofitas BL, Comisel GG, et al. Interventions for pityriasis rosea. Cochrane Database Syst Rev. 2007;(2): CD005068. [CrossRef] [PubMed]
- Chuh, A.A.T., Quality of Life in Children with Pityriasis Rosea: A Prospective Case Control Study. Pediatric Dermatology. 2003, 20: 474-478. [CrossRef] [PubMed]
- Ciccarese, Giulia & Parodi, Aurora & Drago, Francesco. Pediatric pityriasis rosea. TURKISH JOURNAL OF MEDICAL SCIENCES. 2017, 47:1302-1305. [CrossRef] [PubMed]
- Goldstein A.; Goldstein B. Pityriasis Rosea. UpToDate. Retrieved February 22, 2023, from https://www.uptodate.com/contents/pityriasis-rosea.
- Bukhari I. Pityriasis rosea with palmoplantar plaque lesions. Dermatol Online J 2005; 11:27. [CrossRef] [PubMed]
- Browning JC. An update on pityriasis rosea and other similar childhood exanthems. Curr Opin Pediatr. 2009;21(4):481-485. [CrossRef] [PubMed]
- González LM, Allen R, Janniger CK, Schwartz RA. Pityriasis rosea: an important papulosquamous disorder. Int J Dermatol. 2005;44(9):757-764. [CrossRef] [PubMed]
- Neoh CY, Tan AW, Mohamed K, Sun YJ, Tan SH. Characterization of the inflammatory cell infiltrate in herald patches and fully developed eruptions of pityriasis rosea. Clin Exp Dermatol. 2010;35(3):300-304. [CrossRef] [PubMed]
- Rebora A, Drago F, Broccolo F. Pityriasis rosea and herpesviruses: facts and controversies. Clin Dermatol. 2010; 28(5):497-501. [CrossRef] [PubMed]
- Eisman S, Sinclair R. Pityriasis rosea. BMJ. 2015;351:h5233. [CrossRef] [PubMed]
- LOPEZ-CARRERA, Igor et al . Pitiriasis rosada: un exantema que debe ser reconocido por el médico de primer contacto. Estudio de 30 casos. Acta pediatr. Méx. 2014, v.35, n.4, p.289-294. [CrossRef]
- VanRavenstein K, Edlund BJ. Diagnosis and management of pityriasis rosea. Nurse Pract. 2017;42(1):8-11. [CrossRef] [PubMed]
- Schadt C. Pityriasis Rosea. JAMA Dermatol. 2018;154(12):1496. [CrossRef] [PubMed]
- Amer A, Fischer H, Li X. The natural history of pityriasis rosea in black American children: how correct is the "classic" description? Arch Pediatr Adolesc Med. 2007;161(5): 503-506. [CrossRef] [PubMed]
- Chuh A, Zawar V, Lee A. Atypical presentations of pityriasis rosea: case presentations. J Eur Acad Dermatol Venereol. 2005;19:120-6. [CrossRef] [PubMed]
- Ciccarese G, Broccolo F, Rebora A, Parodi A, Drago F. Oropharyngeal lesions in pityriasis rosea. J Am Acad Dermatol. 2017;77(5):833-837. [CrossRef] [PubMed]
- Casani C. Pitiriasis Rosada Recurrente. Rev Pediatr Aten Primaria. 2006;8(6):15-9.
- Cavanaugh RM Jr. Pityriasis rosea in children. A review. Clin Pediatr (Phila). 1983;22(3):200-203. [CrossRef] [PubMed]
- Rodriguez-Zuniga M, Torres N, Garcia-Perdomo H. Effectiveness of acyclovir in the treatment of pityriasis rosea. A systematic review and meta-analysis. An Bras Dermatol. 2018;93(5):686-695. [CrossRef] [PubMed] [PMC free article]
DOI: https://doi.org/10.7199/ped.oncall.2025.34
|
| Cite this article as: | | Dias J P F, Azevedo A C S F d, Vieira C I B, Brito H F d C. Pityriasis Rosea in Children - Cases reports and review. Pediatr Oncall J. 2025;22: 117-120. doi: 10.7199/ped.oncall.2025.34 |
|