The diagnosis of depressed skull fracture (DSF) was considered and skull radiography confirmed an abnormal concavity in the right parietal bone (Figure 2). Cranial ultrasound showed no intracranial hemorrhages (ICH) or cerebral edema. Given his good clinical condition, the newborn was discharged home after 48 hours of hospitalization with weekly neurosurgery follow-up consultations.
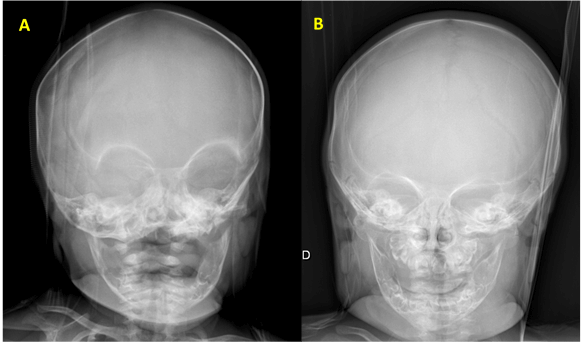
After a 3-week period there was no evident spontaneous remodelling of the skull. Given the fracture’s dimensions, surgical elevation of the bone was performed after parental consent with a good clinical outcome (Figure 3). No post-operative complications were reported and the child showed an adequate growth and neurodevelopment over the first year of life.
Figure 2. Skull radiography after birth showing a concavity in the right parietal bone (arrows).
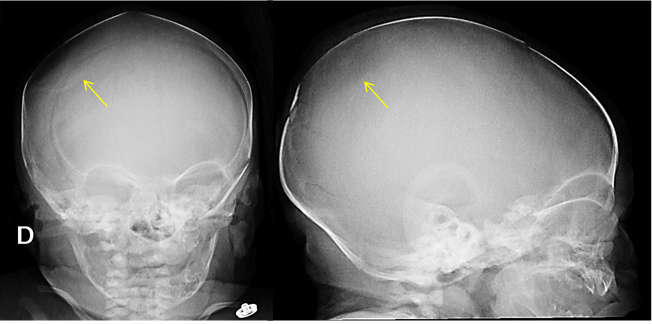 Figure 3.
Figure 3. Skull radiography after surgical elevation of the parietal bone.
A. - One week after surgery.
B - Two months after surgery.
DSF, also called
ping-pong fractures, are a rare condition that occurs in 1-2,5/100.000 neonates. Congenital DSF are commonly associated to birth trauma (instrumentation or maternal bone structures), causing inward buckling of the bones during delivery. Although rare, sometimes they can be observed in newborns following a non-traumatic delivery and are therefore described as spontaneous DSF; these are believed to be caused by prolonged focal pressure on the neonatal skull by structures on the mother’s pelvis (ischial bone, sacral promontory, symphysis pubis, uterine fibroid, the fifth lumbar vertebrae, etc.).
1,2,3 Most cases reported in the literature affect the parietal or frontal bones, as it is believed that the location of the fracture correlates with the presentation of the fetal head to the pelvic inlet.
4 A concavity in a newborn’s skull should always evoque the diagnosis of DSF. Detailed birth history and postnatal examination for evidence of acute injury are crucial to distinguish between spontaneous and traumatic lesions.
Skull radiography often shows the degree of deformation but no fracture line is seen, as there is undisrupted bone continuity.
5 Cranial ultrasound can identify ICH, hematomas or cerebral edema, that are significantly more frequent in DSF secondary to instrumental delivery. Although a computed tomography scan is a more sensitive exam, given the high radiation exposure it should be performed only if there is diagnostic doubt or associated complications.
1 Some rare but serious complications have been described after compound traumatic DSF, such as cerebral contusions, parenchymal lesions and long-term deficits like epilepsy or brain tumours
6,7,8 In the present case, the parietal area was involved without any intracranial pathology or neurological deficits and there was no history of trauma or instrument-assisted delivery, although the fetus was difficult to extract. As there was no local bruising or soft tissue swelling, a traumatic etiology seemed less likely.
Management of this condition is still controversial as there is no standard protocol at the current moment. Since the bone progressively remodels into a normal shape, DSF can be managed expectantly, as described in some previous case reports.
2,3,9,10 Other treatment options include non-surgical interventions, such as digital pressure or vacuum extractor and surgical elevation. The choice is usually based on clinical symptoms, the severity of the fracture and the existence of underlying brain injury or increased intracranial pressure.
3,4
Spontaneous DSF and those affecting children with a normal neurological examination are associated with a good prognosis and most cases resolve spontaneously within the first six months of life.
3,10 It has been suggested that a depression greater than 5 mm on the neonatal skull could lead to a focal area of tissue hypoperfusion and cerebral edema
11; however, a critical measurement has not been yet established to indicate the need for intervention. Corrective surgery may be required when no spontaneous remodeling of the skull is observed or in large lesions with a mass effect on brain structures. Further comments and reports on neonates with DSF may be required to enlighten the most adequate treatment approach for each case.
| References : |
- Preston D, Jackson S, Gandhi S. Non-traumatic depressed skull fracture in a neonate or "ping pong" fracture. BMJ Case Rep. 2015;2015: bcr2014207077.
- Ilhan O, Bor M, Yukkaldiran P. Spontaneous resolution of a 'pingpong' fracture at birth. BMJ Case Rep. 2018;2018: bcr2018226264.
- Sorar M, Fesli R, Gürer B, Kertmen H, Sekerci Z. Spontaneous elevation of a ping-pong fracture: Case report and review of the literature. Pediatr Neurosurg. 2013;48:324-6.
- Veeravagu A, Azad TD, Jiang B, Edwards MSB. Spontaneous intrauterine depressed skull fractures: report of 2 cases requiring neurosurgical intervention and literature review. World Neurosurg 2018; 110: 256-262.
- Lunt CMB, Roth K, Eich G, et al. Neonatal ping pong fracture. Swiss Society of Neonatology, 2006.
- Dupuis O, Silveira R, Dupont C, et al. Comparison of "instrument-associated" and "spontaneous" obstetric depressed skull fractures in a cohort of 68 neonates. Am J Obstet Gynecol 2005;192: 165-70.
- Tervilä L, Huhmar EO, Krokfors E. Cerebral birth injury as a cause of epilepsy. Ann Chir Gynaecol Fenn 1975;64: 118-22.
- Gurney JG, Preston-Martin S, McDaniel AM, et al. Head injury as a risk factor for brain tumors in children: results from a multicenter case-control study. Epidemiology 1996;7:485-9.
- Basaldella L, Marton E, Bekelis K, et al. Spontaneous resolution of atraumatic intrauterine ping-pong fractures in newborns delivered by cesarean section. J Child Neurol 2011;26:1449-51.
- Loire M, Barat M, Mangyanda Kinkembo L, Lenhardt F, M'buila C. Spontaneous ping-pong parietal fracture in a newborn. Arch Dis Child Fetal Neonatal Ed. 2017;102:F160-1.
- Ben-Ari Y, Merlob P, Hirsch M, et al. Congenital depression of the neonatal skull. Eur J Obstet Gynecol Reprod Biol 1986;22: 249-55.
|