Introduction
Coarctation of Aorta is a congenital anomaly of the aorta, which presents as a constriction usually at the junction of the descending aorta and arch of aorta.[1]
Pathogenesis
Coarctation of aorta usually results from defects in the embryonic development of the aortic arch. After birth, the ductus arteriosus constricts to form the ligamentum arteriosum via the contraction of the smooth muscles in the media. If this constriction extends into the aorta, a coarctation ensues.[2]
Also, in fetal life, the majority of the right ventricular output flows through the ductus arteriosus into the descending aorta, while the left ventricular output supplies the upper body. The aortic isthmus, located just between the left subclavian artery and the insertion of the ductus arteriosus, is the narrowest part of the aorta at birth. After birth, when the ductus arteriosus closes, the descending aorta receives all its blood from the left ventricle via the ascending aorta and supplies this blood to the lower part of the body. However, in patients of coarctation of aorta, owing to the constriction, less blood is supplied to the lower half of the body leading to a higher blood pressure in the upper half as compared to the lower half.[1] Such patients are also prone to LV dysfunction and heart failure.
Etiology
- Coarctation of aorta is Seen in 30% of Turner's Syndrome patients.
- M:F=2:1
- 40-80% patients have bicuspid aortic valve
Coarctation of Aorta - Types
- Preductal: When the constriction is before the insertion of the ductus arteriosus, it is also associated with other defects (40%)
- Postductal: When the constriction is after the insertion of the ductus arteriosus
Coarctation of Aorta - Clinical Manifestations
Neonates with severe coarctation of aorta present with symptoms of heart failure like lethargy, poor feeding, respiratory distress, positive suck-rest-suck cycle, forehead sweating while feeding, etc. Older children and adults present with hypertension, headaches, vision problems, intermittent claudication , pain or weakness in legs, especially after exercises like running (in uncomplicated coarctation).[1][2]
Physical Examination:
- Pulse: Pulse: absent, weak or delayed in the femoral as compared to the brachial arteries[1].
- Raised blood pressure in the upper limbs as compared to the lower limbs. A systolic blood pressure gradient of more than equal to 20 mmHg is considered to be indicative of severe coarctation.[2]
- A systolic thrill is usually palpable and carotid pulsations are visible in the suprasternal notch.
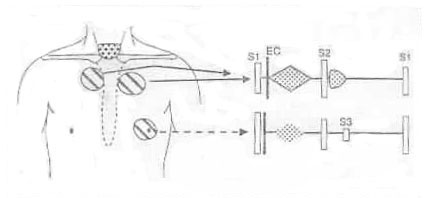
- S1 is accentuated and S2 is normally split with a loud A2.
- Mid-systolic ejection murmur at LLSB and back (right),usually in the interscapular area.
Figure 1: Cardiac findings of coarctation of the aorta. A systolic thrill may be present in the Suprasternal notch (area shown by the dots)
Coarctation of Aorta - Investigations
Physical examination
- A detailed history with proper BP measurement in all four extremities is extremely essential.[2]
ECG
- newborn: RVH
- older child: normal or LVH. ST or T wave changes may be noted in older children that suggest concurrent aortic stenosis or endocardial fibroelastosis[1].
Chest X-ray
- "3 sign" on overpenetrated film representing the prestenotic dilatation, indentation at constriction and poststenotic dilatation[2].
- Aortic knuckle may be appreciated.[1]
- Rib notching- Excessive pressure over the arteries of the upper extremities opens new collaterals. The intercostal vessels enlarge as a result, leading to erosion of surrounding ribs and contributing to rib notching.
Coarctation of Aorta - Treatment
Medical- Initially, the neonate is treated for shock with proper cardio respiratory support. Prostaglandin E1 may be given to reestablish flow in the ductus arteriosus to ease the pressure load over the arteries[2].
Surgical - resection of Coarctation of aorta (4-5 years)
- End-to-end anastomosis - The constricted part is removed and the ends are anastomosed. Now this technique is less employed due to it’s adverse effects.[2]
- Patch grafts - A Dacron graft or a homograft aortic patch is used. But not suitable for growing children due to failure of growth of patch along with the child’s growth[2].
- Left subclavian artery as a patch- This technique has lesser side effects but may cause arm claudication rarely[2].
- Minimally invasive procedures- Aortic Balloon angioplasty and stent placement: A balloon is inserted into the aorta and inflated, which then helps to dilate tge constricted portion. A stent may be placed to keep that part patent[2].
Coarctation of Aorta - Complications
- Systemic hypertension- Coarctation patients are prone to hypertension even after aortic repair. Hypertension increases the risk of cerebrovascular accidents, LVH and heart failure[2].
- Re coarctation- There is a risk of re coarctation in 10-20% patients. This complication is relatively more common in angioplasty procedures[2].
- Aneurysm- Aneurysms may develop at the operated site especially in patients with patch repair. The aneurysm may burst resulting in aortic dissection and high risk of mortality[2].
- Coronary artery disease- There is a slightly more risk of CAD in adulthood in these patients.[2]
- Spinal cord ischemia
- Post-coarctectomy syndrome
1. Ghai’s Textbook of Essential Pediatrics
2. Law MA, Collier SA, Sharma S, Tivakaran VS. Coarctation of the Aorta. 2024 Dec 11. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 28613663.