Transposition Of Great Arteries
Amar Taksande
MD, FIAE, Fellowship in Paed. Cardiology
Jawaharlal Nehru Medical College, Sawangi (Meghe), Wardha
First Created: 01/09/2001
Last Updated: 06/28/2016
Show details
Introduction
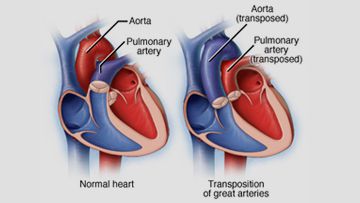
Transposition of the great arteries (TGA) is the common cyanotic congenital heart lesion that presents in neonates. It is ventriculoarterial discordance, in which the aorta arises from the morphologic right ventricle and the pulmonary artery arises from the morphologic left ventricle. The anatomical classifications of TGA depend on the relationship of the great arteries to each other.
Presentation
TGA with intact ventricular septum
- Cyanosis at birth
- The second heart sound is single and loud with no systolic murmur
TGA with large VSD
- Mild cyanosis
- Signs of congestive heart failure may become evident over the first 3-6 weeks
- Palpable right ventricular impulse
- On auscultation, a prominent grade 3-4/6 holosystolic murmur, third heart sound, mid-diastolic rumble, and a gallop rhythm are heard
TGA with VSD and Left ventricular outflow tract Obstruction
- Extreme cyanosis at birth
- A single or narrowly split, diminished S2 and grade 2-3/6 ejection systolic murmur
Investigations
- Severe arterial hypoxemia with or without acidosis
- Hypoglycemia and hypocalcemia are rarely present
- Chest X-ray: Mild Cardiomegaly with narrow upper mediastinum with “Egg on side” appearance of the cardiac shadow (Due to the anteroposterior relationship of the great arteries). Also, there are increased pulmonary vascular markings.
- The electrocardiographic features are a rightward deviation of the QRS complex axis associated with right ventricular hypertrophy; biventricular hypertrophy is evident in conditions that lead to a left ventricular overload.
- Echocardiography: Demonstrate the abnormal vessel connections and associated abnormalities. In the parasternal long-axis view, the arteries arising from the morphologically left ventricle has a posterior course and bifurcates immediately, being recognized as the pulmonary vessel. In the parasternal short-axis view shows the “Circle and Sausage” appearance of the normal great vessels is not visible instead, they appear as “Double Circles”. The pulmonary artery is in the center and the aorta is anterior and to the right of the pulmonary artery.
- CT scan or MR imaging can give some additional details of some associated lesions.
- Prenatal diagnosis by Fetal echocardiography is possible and desirable, as it may improve and useful for the early neonatal management.
Treatment
Medical
- Prostaglandin E1 infusion should be given to improve arterial oxygen saturation by reopening the ductus arteriosus. This is very important in patients with severe left ventricular outflow tract stenosis or atresia. Balloon atrial septostomy (“Rashkinds” Procedure) is a life- saving procedure that may be performed in children with any type of TGA with an intact ventricular septum. The balloon atrial septostomy is used to increase the atrial level shunt and to improve mixing.
Surgical
- Arterial switch operation (ASO): In this surgical operation, the pulmonary artery and aorta are transected above the arterial valves and switched over. Also, the coronary arteries have to be transferred across to the new aorta. Thus the left ventricle act as the systemic ventricle, pumping fully oxygenated blood into the aorta and the right ventricle assumes its normal pumping of blood to the lungs.
- In complex cases of transposition such as in those narrowing below the pulmonary valve, the ASO is not recommended. Alternative approaches are required whenever the arterial switch is not feasible.
- A repair at the atrial level, either by Mustard or Senning procedure, is usually suitable for hearts with an intact ventricular septum.
- If the VSD is large and non-restrictive and the anatomy of the coronary artery makes as an ASO inadvisable, a Rastelli-type of intracardiac repair may be feasible.
Complications
- Congestive heart failure
- Arrhythmia
- Spontaneous cerebrovascular accident in less than 2 year of age
- Brain abscesses in a surgically uncorrected patients older than 2 year of age
- Higher incidences of learning disabilities, speech and language problems, and motor delays
 Amar Taksande
Transposition of Great Arteries
https://www.pediatriconcall.com/show_article/default.aspx?main_cat=pediatric-cardiology&sub_cat=transposition-of-great-arteries&url=transposition-of-great-arteries-introduction
2016-06-28
2016-06-28
Amar Taksande
Transposition of Great Arteries
https://www.pediatriconcall.com/show_article/default.aspx?main_cat=pediatric-cardiology&sub_cat=transposition-of-great-arteries&url=transposition-of-great-arteries-introduction
2016-06-28
2016-06-28
×
Contributor Information and Disclosures
Amar Taksande
MD, FIAE, Fellowship in Paed. Cardiology
Jawaharlal Nehru Medical College, Sawangi (Meghe), Wardha
First Created: 01/09/2001
Last Updated: 06/28/2016