Ventricular Septal Defect - Types
- Supracristal
- Membranous
- Posterior
- Muscular
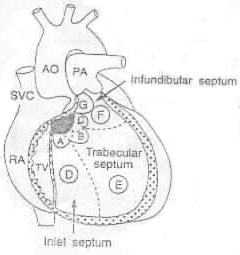
Figure 1: Anatomical locations of various ventricular septal defects, viewed with the right ventricular free wall removed
A= perimembranous inlet (" AV canal - type") VSD
B= Perimembranous trabecular (typical membranous) VSD
C= Perimembranous infundibular ("tetralogy-type") VSD
D= Inlet muscular VSD
E= Trabecular muscular VSD
F= Infundibular (or outlet) muscular VSD
G= Subarterial infundibular ("supracristal") VSD
The black area represents the membranous ventricular septum
Presentation
Small VSD: asymptomatic. Spontaneous closure occurs in 40-50% by 3 years of age
Large VSD: CHF at 2-3 months of age. Diastolic rumble is usually heard.
Physical Examination:
- Poor weight gain
- Systolic thrill with holosystolic murmur at LLSB
- Diastolic murmur with large shunts and loud P2 with pulmonary hypertension
Figure 2: Cardiac findings of a small VSD.
A regurgitant systolic murmur is best audible at the LLSB; it may be holosystolic or less than holosystolic. Occasionally, the heart murmur is in early systole. A systolic thrill (Dots) may be palpable at the LLSB. The S2 splits normally and the P2 is of normal intensity.
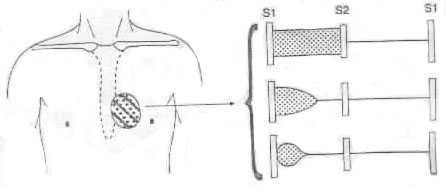
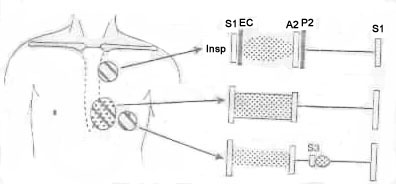
Figure 3: Cardiac findings of a large VSD.
A classic holosystolic regurgitant murmur is audible at the LLSB. A systolic thrill is also palpable in the same area (dots). There is usually a mid-diastolic rumble (due to relative mitral stenosis) at the apex. The S2 is narrowly split and the P2 is accentuated in intensity. Occasionally an ejection click (EC) may be audible in the ULSB when associated with pulmonary hypertension. The heart murmurs shown without solid borders are those murmurs that are transmitted from other areas and are not characteristic of the defect. Abnormal sounds are shown in black.
Investigations
ECG:
- Normal in small VSD
- LAE, LVH in moderate VSD
- LAE, BVH in large VSD
- RVH in Pulmonary vascular obstructive disease (PVOD)
Chest x-ray:
- Heart size: enlarged
- PV: increased
Ventricular Septal Defect - Surgical
- Pulmonary artery banding (done when associated with other defects)
- Direct closure for L-R shunts >2:1 (At 2-4 years of age). It is indicated at any age if CHF not responding to medication or increasing of PVR