Nocardiosis in an immunocompromised child with peripherally inserted central catheter - how to treat?
|
|
Nocardiosis in an immunocompromised child with peripherally inserted central catheter - how to treat?
18/01/2024
18/01/2024
https://www.pediatriconcall.com/Journal/images/journal_cover.jpg
Zahabiya Nalwalla1, Tsering Yangchen Dirkhipa1, Ira Shah1, Venkata Rama Mohan Gollamudi2.
1Department of Pediatric Infectious Diseases, B J Wadia Hospital for Children, Mumbai, India,
2Division of Pediatric Oncology, Department of Medical Oncology, Tata Medical Hospital, Mumbai, India.
ADDRESS FOR CORRESPONDENCE
Tsering Yangchen Dirkhipa, Research Fellow, Department of Pediatric Infectious Diseases, B J Wadia Hospital for Children, Mumbai, India.
Email: tseringyangchen000@gmail.com
Immunocompromised, Peripherally inserted central catheter, Nocardiosis, Indwelling catheter, Nocardia
|
Clinical Problem
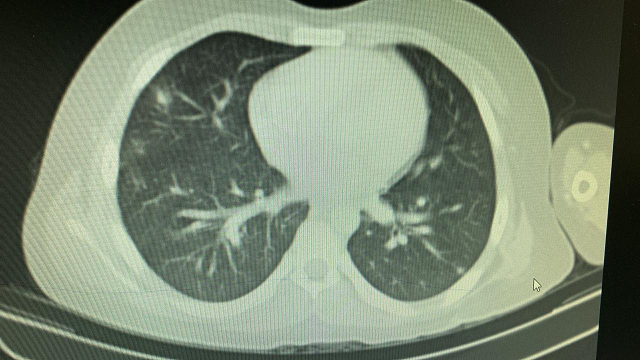
A 12 year old boy was diagnosed as Non-metastatic Ewing’s sarcoma of left scapula in July 2021. He was receiving chemotherapy and a peripherally inserted central catheter (PICC) line was inserted for the same. He presented to us seven months after initiation of chemotherapy with fever for three days and cough with expectoration for 2 days. On examination, weight was 55.3 kg [between 90th and 97th centile as per Indian Academy of Pediatrics (IAP) growth charts], height was 158.2 cm (between 75th and 90th centile as per IAP growth charts). General examination was normal. Examination of the chest revealed crepitations in the right inframammary and infra-scapular area. Other systems were normal. His hemoglobin was 9.1 gm/dl, white cell count was 10,6100 cells/cumm (80% polymorphs, 30% lymphocytes, 20% monocytes, 20% eosinophils) with ESR of 21 mm at end of 1 hour. C-reactive protein (CRP) was 13.6 mg/dl. Chest X-ray showed bilateral lower zone homogenous opacities and CT chest showed multiple new onset nodules in bilateral lung parenchyma with consolidation in right lower lobe measuring 3.1 X 1.9 cm (Figure 1). PICC line and peripheral blood culture grew Nocardia species resistant to amoxicillin-clavulanic acid and ciprofloxacin and sensitive to ceftriaxone, amikacin, linezolid, cotrimoxazole, gentamicin, imipenem and minocycline. MRI brain was done to rule out central nervous system (CNS) dissemination and was normal.
Figure 1. CT Chest showing multiple nodules in bilateral lung parenchyma with a consolidation in the right lower lobe measuring 3.1x1.9 cm.
|
| |
What would be the antibiotic regime for this child? How long do we treat the child? Does the PICC line need to be removed?
|
|
|
Discussion
Nocardiosis is an infection caused by gram positive filamentous bacillus Nocardia spp. The infection as such is uncommon and individuals with an incompetent immune system are the ones susceptible to this ubiquitous organism. Risk factors include poorly controlled HIV infection, patients on long-term corticosteroid treatment, solid organ and hematopoietic stem cell transplant recipients, individuals with malignancy and primary immunodeficiency especially Chronic Granulomatous Disease (CGD).1,2,3 Among these, corticosteroid therapy is considered the most important risk factor for development of nocardiosis.4 Histologically, the organism appears as branching, filamentous and gram positive with weakly acid-fast positive nature. The clinical spectrum varies from cutaneous, pleuropulmonary to disseminated disease. Primary cutaneous results from direct skin inoculation while pleuropulmonary can occur following inhalation of contaminated aerosolized droplets. Either of these can lead to disseminated nocardiosis.2
Primary cutaneous disease presents in the form of abscesses or tender nodules at the site of inoculation while fever, cough, dyspnea or chest pain can be the presenting complaints in pulmonary nocardiosis. When abscess are formed in two or more locations, the disease is considered disseminated with the symptoms based on the area affected.2,5 Disseminated disease has a relatively higher mortality than the former two.1,6 In cancer patients, central venous catheter and peripherally-inserted central catheter (PICC) are two modalities of delivering chemotherapy.7,8 The child in our case had malignancy (Ewing’s sarcoma) and an indwelling PICC for his chemotherapy, thus both increasing his susceptibility to nocardiosis.1,2
In a study by Al Akhrass F and et al, they found that nocardia bacteremia was associated with heavy biofilm formation around the central venous catheter.7 This mechanism may be true for PICC as well since both are indwelling catheters used for long duration. There are multiple conditions which may present similarly such as bacterial pneumonia, tuberculosis, parapneumonic pleural effusion, glioblastoma multiforme and sporotrichosis.1,2 Due to the ubiquitous nature of the organism and rarity of the infection, diagnosis becomes challenging. Hence, high index of suspicion is required.1,2 Initial evaluation should include bacterial culture of the suspected sites and if dissemination or pulmonary infection is suspected, blood culture should be included as well. Chest X-ray and CT scan of chest should be done in case of pulmonary infection along with CT or MRI Brain to rule out CNS dissemination.2 Prompt removal of catheter with antibiotic initiation is found to be effective in case of indwelling-catheter associated Nocardiosis.1,7 In our patient, PICC line was removed.
The treatment consists of a minimum of 6 months of antibiotic therapy which should extend for at least 1 month following resolution of symptoms. In immunocompetent individuals, 6-12 months of treatment is often enough while it may be longer in case of immunocompromised individuals. Nocardia is susceptible to trimethoprim/sulfamethoxazole (TMP-SMX), amikacin, meropenem, third-generation cephalosporins, minocycline, linezolid, amoxicillin-clavulanic acid, dapsone, moxifloxacin and clarithromycin.2 TMP-SMX is the most commonly used first line agent, however the treatment should be individualized and based on culture sensitivity. Monotherapy is sufficient for cutaneous disease in an immunocompetent individual while combination regimen is preferred in case of pulmonary and disseminated disease.2,9 It is advisable to continue monitoring for up to 1 year after antibiotic cessation to detect any relapse.1,7 Our patient was treated with Injection meropenem, linezolid and cotrimoxazole. Meropenem and linezolid were stopped after 2 weeks and cotrimoxazole continued. Repeat cultures after 4 weeks showed no growth with absence of nodules in the CT chest. Treatment was then continued for 6 months with complete recovery of nocardiosis.
The child was followed up for 1 year following the infection. Clinically he was well with no signs of recurrence. He completed chemotherapy for Ewing’s Sarcoma.
|
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
- Watson MEJ, Estabrook MM, Burnham CAD. Catheter-associated Nocardia higoensis bacteremia in a child with acute lymphocytic leukemia. J. Clin. Microbiol. 2011;49(1):469. [CrossRef] [PubMed] [PMC free article]
- Rawat D, Rajasurya V, Chakraborty RK, Sharma S. Nocardiosis. [Updated 2022 Aug 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526075/
- Restrepo A, Clark NM. Infectious Diseases Community of Practice of the American society of Transplantation. Nocardia infections in solid organ transplantation: guidelines from the Infectious Diseases Community of Practice of the American Society of Transplantation. Clin Transplant 2019;33:e13509. [CrossRef] [PubMed]
- Leite IM, Trigueiros F, Martins AM, Fonseca M, Marques T. Disseminated Nocardiosis: A Case Report. Cureus. 2019 Aug 1;11(8):e5294. doi: 10.7759/cureus.5294. PMID: 31588382; PMCID: PMC6771935. [CrossRef]
- Tomas RM, Villanueva RM, Calzada SR, Durantez MS, Tarazona JMV, Alapont MM, Serrano MG. Pulmonary nocardiosis: risk factors and outcomes. Respirology. 2007;12(3):394-400. [CrossRef] [PubMed]
- Williams E, Jenney AW, Spelman DW. Nocardia bacteremia: A single-center retrospective review and a systematic review of the literature. Int J Infect Dis. 2020;92:197-207. doi: 10.1016/j.ijid.2020.01.011. [CrossRef] [PubMed]
- Al Akhrass F, Hachem R, Mohamed JA, Tarrand J, Kontoyiannis DP, Chandra J, Ghannoum M, Haydoura S, Chaftari AM, Raad I. Central venous catheter-associated Nocardia bacteremia in cancer patients. Emerg Infect Dis. 2011 Sep;17(9):1651-8. doi: 10.3201/eid1709.101810. PMID: 21888790; PMCID: PMC3322064. [CrossRef] [PubMed] [PMC free article]
- Sapkota S, Sannur R, Naik R. Analysis of Peripherally Inserted Central Catheter Line in Cancer Patients: A Single-Center Experience. South Asian J Cancer. 2020 Oct;9(4):253-256. doi: 10.1055/s-0040-1721175. Epub 2021 Jun 15. PMID: 34141688; PMCID: PMC8205555. [CrossRef] [PubMed] [PMC free article]
- Aggarwal D, Garg K, Chander J, Saini V, Janmeja AK. Pulmonary nocardiosis revisited: A case series. Lung India. 2015 Mar-Apr;32(2):165-8. doi: 10.4103/0970-2113.152638. PMID: 25814804; PMCID: PMC4372873. [CrossRef] [PubMed] [PMC free article]
|
|
| |
Cite this article as:
Nalwalla Z, Dirkhipa T Y, Shah I, Gollamudi V R M. Nocardiosis in an immunocompromised child with peripherally inserted central catheter - how to treat?. Pediatr Oncall J. 2024;21: 41-42. doi: 10.7199/ped.oncall.2024.12
|