Sarah M. Alfaqaih1,2, Mohamed Bashaga2,3, Yaser Omar Howayw4.
1Pediatric Oncology Department, National Cancer Institute, Misurata, Libya,
2Faculty of Medicine, University of Misurata, Libya,
3Diagnostic Radiology department, National cancer institute, Misurata, Libya,
4Oral and Maxillofacial Department, Misurata Medical Center, Misurata, Libya.
ADDRESS FOR CORRESPONDENCE
Sarah M. Alfaqaih, 2478, Misurata, Libya
Email: sarah.alfaqaih@med.misuratau.edu.ly | | Abstract | Background: Cherubism is a rare autosomal dominant inherited disorder, caused by a mutation in the SH3BP2 gene. imatinib has been effectively reported as an option of treatment. imatinib, a tyrosine kinase inhibitor (TKI), has been established to promote osteoblast differentiation. According to our knowledge, this is the first reported case of cherubism in Libya that suggest effectivity of imatinib.
Case presentation: We present the case of a 4-year-old boy was diagnosed with cherubism. The child was consistently administered a daily oral dosage of imatinib (300 mg/m2) for three months. Throughout the treatment, the patient was closely monitored every two weeks for potential side effects and signs of clinical improvement.
Conclusion: The observed therapeutic potential of imatinib for cherubism in this case study suggests a promising avenue for future exploration. However, further research is needed to establish a safe and effective protocol for imatinib treatment in pediatric cherubism. | | | | Keywords | | Tyrosine kinase inhibitor, Cherubism, imatinib, Non-familial cherubism, SH3BP2 gene. | | | | Introduction | Cherubism (Online Mendelian Inheritance in Man, "OMIM #118400") is a rare genetic disorder inherited in an autosomal dominant manner. It is caused by a mutation in the SH3BP2 gene, which leads to painless enlargement of the mandibular bones. This enlargement is due to a fibrous granuloma containing multinucleated giant cells that can express and differentiate into activated osteoclast giant cells, dependent on or independent of RANK.1,2 The condition was first identified by Jones in 19333 and typically presents in childhood, gradually growing until puberty and then slowly regressing until around the age of 30.4 Treatment options have been described, including observation, reconstructive surgery and pharmacological therapy.5 Kueper, et al.6, from a systemic review of published literature, analyze data including 92 individuals from 34 families diagnosed with cherubism. Only 15% of the included individuals have no family history of cherubism, which mostly became clinically evident between 5 and 9 years of age. The surgical approach to treatment was mostly followed for cases receiving lesion curettage and recontouring; some cases showed no sign of recurrence during one year of follow-up, while on the other hand, some cases showed aggressive signs of disease progression.
In our case, we report the results of imatinib for cherubism regarding efficacy and safety. To the best of our knowledge, only three patients have been treated with imatinib, as reported in the literature.7 | | | | Case Report | In October 2022, a 4-year-old boy with no family history of the disease presented with bilateral ear discomfort and cheek fullness over a three-month duration. He was referred for further evaluation. Physically, he has bilateral painless swelling of the cheekbones, no palpable lymph nodes and a pre-pubertal tanner stage. His height (106 cm, 75the percentile), weight (17.8 kg, 75the percentile) and body mass index (15.8/m2, 50the percentile) met normal developmental milestones and he was fully vaccinated under the national vaccination program.
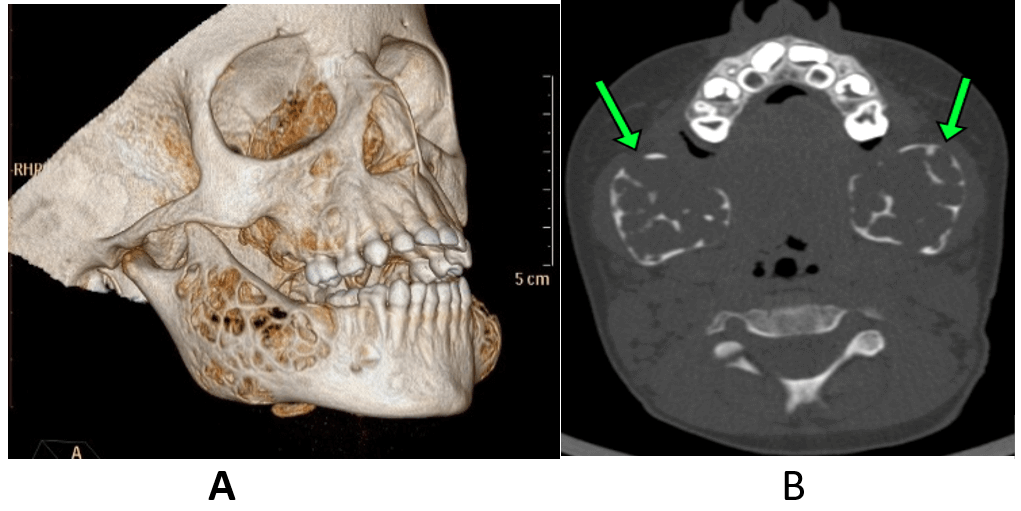
The baseline laboratory normal, including complete blood count and bone profile, is shown in Table 1. An imaging computerized tomography scan showed symmetric bilateral mandibular bone expansible lytic lesions with internal trabeculations, giving the soap bubble appearance, involving the mandibular bodies and rami, sparing the condyles (Figure 1). Cherubim Grade-I, according to the Seward and Hankey grading system.8
Table 1. Baseline and follow-up laboratory profile.
| Variant |
Initial |
Week 6 |
Week 12 |
Post treatment |
| Hb g/dl |
11.2 |
10.9 |
11.3 |
10.7 |
| WBC × 103 |
7.7 |
5.5 |
7.8 |
7.8 |
| Lymphocyte % |
38 |
54 |
39.4 |
40.4 |
| Granulocyte % |
45 |
31 |
53.4 |
51.3 |
| Mix % |
16 |
15 |
7.6 |
8.3 |
| Platelet ×103 |
266 |
361 |
100 |
236 |
| ALT U/l |
8 |
13 |
11 |
10.7 |
| AST U/l |
25 |
35 |
35 |
22.1 |
| ? GT U/l |
- |
10 |
10 |
|
| Bilirubin (T/D) mg/dl |
0.1/- |
0.8/0.1 |
0.3/0.1 |
0.24/0.1 |
| Lipase U/l |
20 |
96 |
19 |
|
| Amylase U/l |
105 |
22 |
119 |
|
| Alk. Ph U/l |
150 |
114 |
141 |
|
| LDH U/l |
273 |
347 |
227 |
239 |
| Total protein g/l |
6.1 |
6.2 |
6.8 |
|
| Serum albumin g/l |
4.1 |
3.7 |
3.8 |
|
| PTH |
27.9 |
|
|
|
| Vitamin D |
28 |
|
|
35 |
ALT: alanine aminotransferase, AST: aspartate aminotransferase, ? GT: gamma-glutamyl transferase, Alk. Ph: alkaline phosphatase, LDH: lactate dehydrogenase, PTH: parathyroid hormone
Figure 1. A, 3D reconstruction; B, axial CT scan shows bilateral mandibular bone expansible lytic with internal trabeculations at presentation.
We diagnosed the child with cherubism upon clinical and detailed radiological evaluation. The parents have been counseled about the natural history of the disease and treatment options and trials, including waiting and follow-up, surgical intervention and drugs (imatinib). His family wished to start noninvasive treatment.
This study approved by the National Cancer Institute Misurata’s ethical Committee (No. 02-133/2023). We obtained parents’ written consent for treatment and for publishing the pictures and treatment results. imatinib, 300 mg/m2 by mouth daily (rounded to the nearest tablet), was 200 mg daily. The patient was treated consistently for three months without interruption. He followed up every two weeks to closely monitor side effects and signs of clinical improvement. The patient tolerates treatment well apart from occasional nausea, which oral ondansetron controls. By week 10 of the treatment course, complete blood counts showed thrombocytopenia (platelet count 100-103), which recovered spontaneously without modification of dosage. The comparative imaging study pre- and post-introduction of imatinib showed the mandibular thickness measured 1.7 cm" as compared to 3.0 cm" in the previous study, with still a few trabeculations and a response rate of 43% (Figure 2 A, B). The follow-up imaging scan eight months post treatment showed a further response although cessation of imatinib treatment with response > 60% compared with initial scans (Figure 3 A, B).
Figure 2. A, 3D reconstruction; B, axial CT scan shows the regressive course of the lesion 3 months post imatinib treatment.
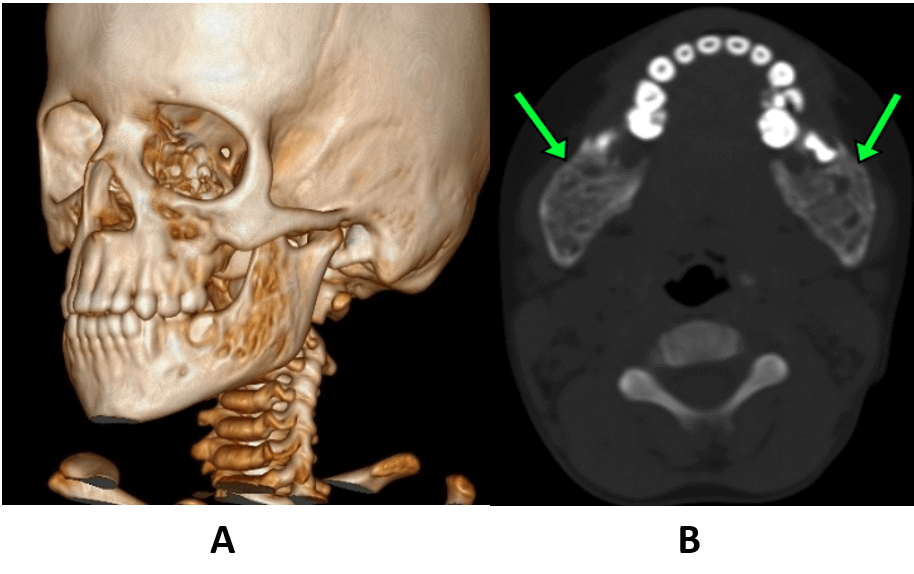
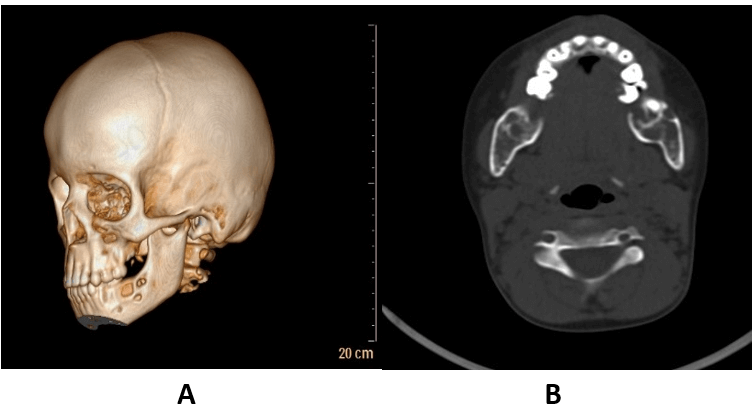
Figure 3. A, 3D reconstruction; B, axial CT scan shows the regressive course of the lesion 8 months post imatinib treatment.
The patient's growth curves have been unaffected over eight months of follow-up. At the last follow-up, he did not show any sign of recurrence.
| | | | Discussion | The treatment options for cherubism raise several dilemmas for the treating physician, as expected of self-limiting and usually involuntary consequences of treatment effects.9,10 On the other hand, the early aggressive course of the disease and the major disfigurement and functional complications indicate a search for a minimally invasive modality of treatment.7,11,12,13 The surgical intervention is the typically reported first-line module of treatment for symptomatic and plastic surgery.4,14,15 For severe cases, the timing of intervention and surgical approach remain the most challenging parts for surgeons.15
As a consequence, several pharmacological treatment trials (for instance, imatinib, denosumab, calcitonin, tacrolimus, alodronate and adalimumab) have been reported for the limited number of cases, but no established guidelines for treatment have been reached.12,13,16,17,18,19,20
We report a case of cherubism in a prepubertal age, in which imatinib was administered as a therapeutic intervention. The rationale for prescribing imatinib is grounded in its demonstrated capacity to promote osteoblastogenesis by inhibiting platelet-derived growth factor.21 The definite mechanism of action is not well established.22,23 The administration of imatinib was chosen due to the parents' unwillingness to make alternative therapeutic choices. Parents and physician were aware of minor and serious side effects reported. imatinib has demonstrated favorable results in several cases pertaining to the management of cherubism and clinically similar occurrences of Central Giant Cell Granuloma of the Jaw (CGCGJ).7,24
Imatinib, a tyrosine kinase inhibitor (TKI), has been effective in treating many childhood disorders, including chronic myelogenous leukemia (CML) and acute lymphoblastic lymphoma (Ph+ ALL, Philadelphia chromosome positive). This provides a solid foundation for its ongoing utilization. Children often exhibit good tolerance to the therapy, which can last from 24 to 60 months. Nevertheless, there have been documented instances of adverse effects, including bone marrow suppression, nausea, muscular cramps, diarrhea, edema, hepatotoxicity, dermatitis and growth inhibition in prepubescent children.25 It is important to mention that the inhibition of growth often resolves with puberty.26 Several reports on its effects on male and female fertility.27
In this report, a three-month treatment with imatinib resulted in a significant reduction of the lesion with new bony ossification of osteolytic lesions. The patient reported a minor side effects includes an occasional nausea with initiation of imatinib which effectively controlled with ondansteron and thrombocytopenia which require no dose modification. Ricalde et al.7, report three cases ("case 1," a 6-year-old boy; "case 2," a 6-year-old boy; "case 3," a 4-year-old girl) that have been treated with imatinib for at least 6 months of consistent treatment for a severe form of cherubism. Two cases underwent surgical debulking and tumor relapse before the initiation of treatment. They had treatment responses of 65%, 22% and 75%, respectively, with reductions in tumor volume, no significant side effects reported except for nausea and no reported effect on linear growth. Although they comment on partial compliance and difficult follow-up for treated cases, these results indicate that imatinib may have therapeutic potential for cherubism.
Denosumab is an inhibitor of the RANK ligand, which significantly suppresses the differentiation, proliferation and activation of osteoclasts.28 denosumab has been reported in the literature as a possible pharmacological therapy for cherubism. Four cases ("Case 1," a 9-year-old boy; "Case 2," a 19-year-old female; "Case 3," a 15-year-old female; and "Case 4," a 5-year-old female) from three published studies have been treated with denosumab.13,29,30 Duration of treatment ranges from 6-12 months in which the response of treatment ranges from the dramatic clinical and radiographic response for pre-pubertal “cases 1, 4” and radiographic response without clinical effect on older ages “case 2, 3”. In addition, significant toxicity associated with denosumab in the form of hypocalcemia may be asymptomatic “ case 1”13 or high-grade hypocalcemia requires hospitalization and modified subsequent doses and spacing e.g. “case 4”.30 An acute renal injury with hyperkalemia has been reported in patients treated with denosumab.31 Also as a consequence of denosumab toxicity on the growth rate, it showed a decreased effect on growth for pre-pubertal age “case 1: after initiation of treatment and after 5 months from the end of therapy.13 There were no significant adverse events reported for “case 2, 3”.29
It has been reported that calcitonin is a feasible option for treatment for a severe form of central giant cell granuloma (CGCG). The rationale for administration is that it inhibits the osteoclastic activity of the giant cells and theoretically should have an effect on cherubism as the lesions are histologically indistinguishable from those in central giant cell granuloma and the bone resorption by the multinucleate cells of cherubism is reduced by calcitonin in vitro.32 There is limited data regarding calcitonin therapy for cherubism. Etoza et al.11 And Lange et al.33, two cases of cherubism (“case 1,” a 14-year-old boy; “case 2,” a 10-year-old boy) treated with salmon calcitonin nasal administration 200 IU for 30 months and 15 months, respectively, post-surgical reconstructive approach for both cases. A significant radiographic response has been reported for “case 1”. In the second case, the lesions were stable and showed no regression for the first 12 months. After 15 months, an initial regression was noticed and the therapy was terminated. The control CT scan, three months after cessation of therapy, showed a considerable regression of the lesions and a restoration of the normal contour of the mandible. There were no considerable side effects reported in either case.
Kadlub et al.18 reported a 2-year-old with severe progressive cherubism with complete obstructive nostrils, enlarged mandibular lymph nodes and orbital compression. Initially, a multiple decompression surgical approach was performed. tacrolimus was introduced at the age of 4 years in two oral doses (0.15 mg/kg/day). After 12 months of initiation of treatment, a clinical improvement was documented by regression of lymph node enlargement, eruption of permanent teeth and stabilization of tumor growth.
Bradley et al.16 have presented a 12-year-old boy treated with oral alendronic acid 70 mg weekly as an adjuvant treatment to surgical debulking for severe cherubism. The duration of treatment initially continued for six months. After 24 months of evaluation, there was a slight progression of the maxillary lesion and a restart of treatment with alendronate for another 12 months, with no final result reported. No significant side effects of treatment were reported during the course of therapy (Table 2).
Table 2. Literature review on cherubism pharmacological therapy.
| Author name/country |
No. of cases |
Age(year) |
Gender |
Treatment protocol |
Follow-up (months) |
Results |
| Bradley, et al. (2020), UK.16 |
1 |
3 |
M |
Alendronic acid, 70 mg PO weekly (*) |
36 |
Limiting the need for more radical surgery |
| Kawamura, et al. (2020), Japan.13 |
1 |
9 |
M |
Denosumab. s/c (120 mg/dose) at days 0, 7, and 28, and then every 4 weeks thereafter for 6 months |
12 |
Maybe a therapeutic option for extensive and aggressive cherubism |
| Droma, et al. (2020), Israel.29 |
2 |
19,15 |
F |
Denosumab, administered subcutaneously in 120 mg doses on days 1, 8, 15, and 28 and then every 28 days |
15 |
A response to treatment was evident within 3 months |
| Ricalde, et al. (2019), USA.7 |
3 |
6,8,4 |
(1,2) M
(3) F |
Imatinib, 300 mg/m2, PO daily dose (*) |
24, 5, 10 respectively |
Significant reduction of size by 75,22,65% respectively |
| Upfill-Brown, et al. (2019), USA.30 |
1 |
12 |
F |
Denosumab, administered subcutaneously in 120 mg doses monthly doses |
24 |
The therapy results in significant clinical and radiographic improvement for pediatric patients. |
| Kadlub, et al. (2014), France.18 |
1 |
4 |
M |
Tacrolimus, two oral daily doses (0.15 mg/kg/day) with target trough level was 5 ng/mL (*)
| 12 |
Showed enhanced bone formation by stimulating osteogenesis |
| Hero, et al. (2012), Finland.12 |
2 |
(1) 7.3
(2) 4.8 |
(1) M
(2) F |
Adalimumab, 40 mg s/c every 2 weeks, for 2 years and 3 months (Patient 1) and 2 years and 7 months (Patient 2) |
30 |
Does not appear to provide sufficient amelioration for patients |
| Etoz, et al. (2011), Turkey.11 |
1 |
14 |
M |
Salmon calcitonin, using a nasal spray of 200 IU |
30 |
Significant radiographic improvement was observed |
| Lange, et al. (2007), Netherlands.33 |
1 |
11 |
M |
Salmon calcitonin, using a nasal spray of 200 IU |
36 |
After 15 months, an initial regression reported |
s/c: subcutaneously, (*): adjuvant therapy with surgical debulking , F=female, M=male.
Anti-tumor necrosis factor (TNF-α antagonist) treatment in cherubism has been reported in the literature by Hero et al.12 Two children, a 7.3-year-old boy and a 4.8-year-old girl, were treated for 2.5 years duration with adalimumab. After a course of treatment, reported cases did not respond to adalimumab. TNF-α antagonists may alter the formation of pathogenic giant cells but do not affect active cherubism.12
| | | | Conclusion | | The observed therapeutic potential of imatinib for cherubism in this case study suggests a promising avenue for future exploration. However, further research is needed to establish a safe and effective protocol for imatinib treatment in pediatric cherubism. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Ueki Y, Lin CY, Senoo M, Ebihara T, Agata N, Onji M, Saheki Y, Kawai T, Mukherjee PM, Reichenberger E et al: Increased myeloid cell responses to M-CSF and RANKL cause bone loss and inflammation in SH3BP2 "cherubism" mice. Cell 2007, 128(1):71-83. [CrossRef]
- Kittaka M, Yoshimoto T, Hoffman H, Levitan ME, Ueki Y: RANKL-independent osteoclastogenesis in the SH3BP2 cherubism mice. Bone Rep 2020, 12:100258. [CrossRef]
- Jones WA: Familial Multilocular Cystic Disease of the Jaws. American Journal of Cancer 1933, 17:946-950. [CrossRef]
- Papadaki ME, Lietman SA, Levine MA, Olsen BR, Kaban LB, Reichenberger EJ: Cherubism: best clinical practice. Orphanet J Rare Dis 2012, 7 Suppl 1(Suppl 1):S6. [CrossRef]
- Ahmadzadeh K, Vanoppen M, Rose CD, Matthys P, Wouters CH: Multinucleated Giant Cells: Current Insights in Phenotype, Biological Activities, and Mechanism of Formation. Front Cell Dev Biol 2022, 10:873226. [CrossRef]
- Kueper J, Tsimbal C, Olsen BR, Kaban L, Liao EC: SH3BP2-related fibro-osseous disorders of the maxilla and mandible: A systematic review. Int J Oral Maxillofac Surg 2022, 51(1):54-61. [CrossRef]
- P R, I A, ST S: A Paradigm Shift in the Management of Cherubism? A Preliminary Report Using Imatinib. In., vol. 77. United States; 2019: 1278.e1271-1278.e1277. [CrossRef]
- Seward GR, Hankey GT: Cherubism. Oral Surg Oral Med Oral Pathol 1957, 10(9):952-974. [CrossRef]
- J K, C T, BR O, L K, EC L: SH3BP2-related fibro-osseous disorders of the maxilla and mandible: A systematic review. International journal of oral and maxillofacial surgery 2022, 51(1):54-61. [CrossRef]
- CH K, NM S, JD E, SG K, ME W: The surgical and orthodontic management of cherubism in a growing child. In., vol. 40. Scotland; 2012: 229-233. [CrossRef]
- OA E, D D, O G: Treatment of cherubism with salmon calcitonin: a case report. European journal of dentistry 2011, 5(4):486-491. [CrossRef]
- M H, A S, J H, P S, R K, H A, S A, S T-S, P L, O M: Anti-tumor necrosis factor treatment in cherubism--clinical, radiological and histological findings in two children. In., vol. 52. United States; 2013: 347-353. [CrossRef]
- H K, S W, T I, I A, H M, S D: Efficacy and safety of denosumab treatment in a prepubertal patient with cherubism. In., vol. 33. Germany; 2020: 963-966. [CrossRef]
- Erratum: Severe Cherubism Treated with Curettage, Osteotomy, and Bony Repositioning: A Case Series of Three Patients-Erratum, vol. 10. United States; 2022. [CrossRef]
- S J, J S, A S, P S: Surgical Treatment of Cherubism With the Use of ThreeDimensional Virtual Planning and CAD-CAM Resection Guides: A Case Report and Systematic Literature Review. In., vol. 33. United States; 2022: 1502-1506. [CrossRef]
- D B, V P, C H, M M: Adjuvant Alendronic Acid in the Management of Severe Cherubism: A Case Report and Literature Review. In., vol. 79. United States; 2021: 598-607. [CrossRef]
- SI L, I CH, L A: Denosumab Therapy in Cherubism. The Cleft palate-craniofacial journal : official publication of the American Cleft Palate-Craniofacial Association 2022:10556656221113891.
- N K, MP V, L G, AC LH, L D, T U, B F, I P, C B, S M et al: The calcineurin inhibitor tacrolimus as a new therapy in severe cherubism. In., vol. 30. United States; 2015: 878-885. [CrossRef]
- M FG, L FdBPF, CM H, F AC, M CA: Clinical and surgical management of an aggressive cherubism treated with autogenous bone graft and calcitonin. In., vol. 2011. Egypt; 2011: 340960. [CrossRef]
- I P, G S, M M, T G, L P, R C: Ineffectiveness of tumor necrosis factor-alpha inhibition in association with bisphosphonates for the treatment of cherubism. In., vol. 29. Italy; 2011: 147.
- Yoshitaka T, Ishida S, Mukai T, Kittaka M, Reichenberger EJ, Ueki Y: Etanercept administration to neonatal SH3BP2 knock-in cherubism mice prevents TNF-α-induced inflammation and bone loss. J Bone Miner Res 2014, 29(5):1170-1182. [CrossRef]
- VM C, PF P, FR A, PE dS, L DM, RS G: Novel mutations in the SH3BP2 gene associated with sporadic central giant cell lesions and cherubism. Oral diseases 2009, 15(1):106-110. [CrossRef]
- Bader-Meunier B, Van Nieuwenhove E, Breton S, Wouters C: Bone involvement in monogenic autoinflammatory syndromes. Rheumatology (Oxford) 2018, 57(4):606-618. [CrossRef]
- B T, RJ P, C M, AKM F, Z F, J B: Response of Central Giant Cell Granuloma of the Jaw to Imatinib. Journal of pediatric hematology/oncology 2022.
- Hochhaus A, Larson RA, Guilhot F, Radich JP, Branford S, Hughes TP, Baccarani M, Deininger MW, Cervantes F, Fujihara S et al: Long-Term Outcomes of Imatinib Treatment for Chronic Myeloid Leukemia. N Engl J Med 2017, 376(10):917-927. [CrossRef]
- Marcucci G, Perrotti D, Caligiuri MA: Understanding the molecular basis of imatinib mesylate therapy in chronic myelogenous leukemia and the related mechanisms of resistance. Commentary re: A. N. Mohamed et al., The effect of imatinib mesylate on patients with Philadelphia chromosome-positive chronic myeloid leukemia with secondary chromosomal aberrations. Clin. Cancer Res., 9: 1333-1337, 2003. Clin Cancer Res 2003, 9(4):1248-1252.
- Rambhatla A, Strug MR, De Paredes JG, Cordoba Munoz MI, Thakur M: Fertility considerations in targeted biologic therapy with tyrosine kinase inhibitors: a review. J Assist Reprod Genet 2021, 38(8):1897-1908. [CrossRef]
- Baron R, Ferrari S, Russell RG: Denosumab and bisphosphonates: different mechanisms of action and effects. Bone 2011, 48(4):677-692. [CrossRef]
- E BD, G B-R, A I, Y F, C A-D, N L, N G: Positive Outcomes of Denosumab Treatment in 2 Patients With Cherubism. In., vol. 78. United States; 2020: 2226-2234. [CrossRef]
- A U-B, S B, NM B, AL F, SD N, A S, K W-P, FC E, NC F: Use of Denosumab in Children With Osteoclast Bone Dysplasias: Report of Three Cases. JBMR plus 2019, 3(10):e10210. [CrossRef]
- Uday S, Gaston CL, Rogers L, Parry M, Joffe J, Pearson J, Sutton D, Grimer R, Högler W: Osteonecrosis of the Jaw and Rebound Hypercalcemia in Young People Treated With Denosumab for Giant Cell Tumor of Bone. J Clin Endocrinol Metab 2018, 103(2):596-603. [CrossRef]
- R B, AM M, A C: [A diagnostic protocol in cherubism]. In., vol. 47. Italy; 1998: 447-451. [CrossRef]
- J dL, HP vdA, M S: Cherubism treated with calcitonin: report of a case. In., vol. 65. United States; 2007: 1665-1667. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2026.64
|
| Cite this article as: | | Alfaqaih S M, Bashaga M, Howayw Y O. The efficacy and safety of imatinib therapy in a case of non-familial cherubism. Pediatr Oncall J. 2026;23. doi: 10.7199/ped.oncall.2026.64 |
|