André Salvada1, Mariana Fidalgo Silva1, Andreia Filipa Mota1, Francisca Costa1, Susana Rocha2, Luís Rito Cruz3, Paula Correia1, Catarina Luís1.
1Child and Youth Department, Unidade Local de Saúde de Amadora/Sintra, Amadora, Portugal,
2Pediatrics Department, Unidade Local de Saúde do Arco Ribeirinho, Barreiro, Portugal,
3Neuroradiology Department, Unidade Local de Saúde de Amadora/Sintra, Amadora, Portugal.
ADDRESS FOR CORRESPONDENCE
André Salvada, Hospital Professor Doutor Fernando Fonseca, IC 19 276, 2720-276, Amadora, Portugal.
Email: andre.salvada@ulsasi.min-saude.pt | | Abstract | Epstein-Barr virus (EBV) infection can lead to complications such as encephalitis, even in immunocompetent individuals.
A previously healthy eight-year-old girl presented with a prodrome of fever, headache, and vomiting. After two days she had a tonic-clonic seizure that evolved to status epilepticus, which resolved with propofol. A diagnosis of probable EBV encephalitis was assumed after detection of EBV DNA in cerebrospinal fluid. Rising copies of EBV DNA were detected in the plasma. Neuroimaging showed focal cortical involvement of the posterior region of the left frontal lobe and of the inferior pole of the ipsilateral temporal lobe. She was treated with acyclovir and showed a full recovery.
EBV encephalitis is a challenging diagnosis due to non-specific clinical manifestations that may significantly overlap with other central nervous system infections. | | | | Keywords | | Human Herpesvirus 4, Epstein-Barr Virus, Encephalitis, Status Epilepticus, Child | | | | Case Report | A previously healthy eight-year-old girl was admitted to the emergency room due to a short afebrile generalized tonic-clonic seizure on the day of admission (under five minutes). One week prior to admission she had a self-limited episode of fever and headache that lasted for three days. Two days before admission fever, headache and vomiting developed. The parents did not recall any symptoms of altered mental status before the day of admission. She had been in contact with several other children with respiratory symptoms at school, in the previous two weeks. Her twin sister also had a self-limited episode of fever and headache the week before admission.
Whilst she was in the emergency room, she had another afebrile generalized tonic-clonic seizure, with upward eye deviation. Pupils were isochoric and photoreactive. After the first 0.5 mg/kg dose of rectal diazepam, the patient developed respiratory depression necessitating invasive mechanical ventilation. She progressed to status epilepticus, leading to the sequential administration of 0.2 mg/kg of midazolam and 40 mg/kg of levetiracetam, without clinical response. The seizures only ceased after starting a propofol infusion at 2 mg/kg/hour. Additionally, ceftriaxone and acyclovir were empirically administered. She was started on levetiracetam 20 mg/kg/day.
Blood analysis on the day of admission showed leukocytosis with neutrophilia and a C-reactive protein (CRP) of 1.81 mg/dL (Table 1). Brain computerized tomography (CT) and chest x-ray post-intubation were unremarkable.
Cerebrospinal fluid (CSF) testing on admission showed a WBC count of 86/mm3 (67% mononuclear cells), rare red blood cells/mm3, glucose 74 mg/dL (serum glucose of 98 mg/dL; CSF/serum glucose ratio of 0.75) and protein of 38.26 mg/dL (Table 1).
Table 1. Laboratory workup.
| Blood analysis on admission |
| Hemoglobin |
12.0 g/dL |
| White blood cell count |
14.9 x 109/L |
| Neutrophil count |
12.8 x 109/L |
| Lymphocyte count |
1.07 x 109/L |
| Platelet count |
305,000 /µL |
| C-reactive protein |
1.81 mg/dL |
| Cerebrospinal fluid (CSF) analysis |
| White blood cells |
86 /mm3 |
| Red blood cells |
rare /mm3 |
| Glucose |
74 mg/dL |
| Serum glucose |
98 mg/dL |
| CSF/serum glucose ratio |
0.75 |
| Protein |
38.26 mg/dL |
| Multiplex PCR CSF meningoencephalitis panel |
| Escherichia coli K1 |
Negative |
| Escherichia coli K1 |
Negative |
| Haemophilus influenzae |
Negative |
| Listeria monocytogenes |
Negative |
| Neisseria meningitidis |
Negative |
| Streptococcus agalactiae |
Negative |
| Streptococcus pneumoniae |
Negative |
| Herpes simplex virus 1, 2 and 6 |
Negative |
| Human parechovirus |
Negative |
| Varicella zoster virus |
Negative |
| Cryptococcus neoformans |
Negative |
| Cryptococcus gattii |
Negative |
| Mycoplasma pneumoniae PCR in CSF |
Negative |
| Epstein-Barr virus PCR in CSF |
Positive |
| CSF culture |
Negative |
| Plasma serologies |
| Mycoplasma pneumoniae |
IgM positive / IgG negative |
| Cytomegalovirus |
IgM negative / IgG positive |
| Borrelia burgdorferi |
Negative |
| Parvovirus B19 |
Negative |
| Human immunodeficiency virus I/II |
Negative |
| Hepatitis B virus |
Negative |
| Hepatitis C virus |
Negative |
| anti-Epstein-Barr virus viral capsid antigen |
IgM negative / IgG positive |
| anti-Epstein-Barr virus nuclear antigen |
IgG positive |
| Epstein-Barr virus PCR in plasma |
Positive |
| Nasopharyngeal PCR panel |
| SARS-CoV-2 |
Negative |
| Influenza A and B |
Negative |
| Respiratory Syncytial Virus |
Negative |
| Autoimmunity plasma screen |
| Antinuclear antibodies (ANA) |
Positive, anti-nucleolar homogeneous pattern
(AC-8, titer of 1:160) |
| Antiganglioside antibodies (AGA) IgM |
Weakly positive for GM3 and GQ1b |
| Antiganglioside antibodies (AGA) IgG |
Negative |
| Rheumatoid factor |
Negative |
| Anticardiolipin antibodies |
Negative |
Serial electroencephalograms (EEG) starting on day one of admittance showed frontal intermittent rhythmic delta activity (FIRDA) and diffuse brain dysfunction.
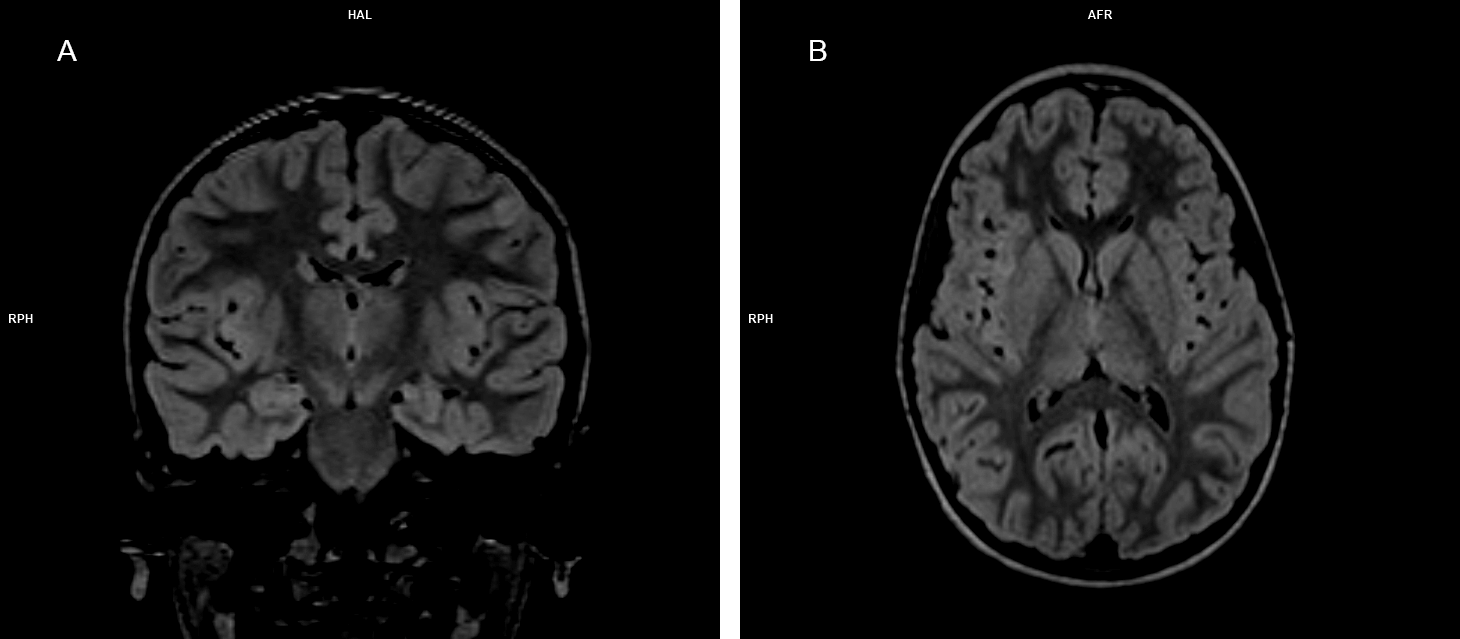
Brain magnetic resonance imaging (MRI) on the 3rd day of admittance showed predominantly cortical left frontal posterior and ipsilateral inferior temporal polar small T2/FLAIR hyperintensities, with no other abnormalities reported (Figure 1).
Figure 1. Brain magnetic resonance fluid-attenuated inversion-recovery (FLAIR) images. (A) Coronal view showing a cortical left frontal posterior hyperintense lesion. (B) Axial view showing unaffected basal ganglia.
Epstein-Barr virus (EBV) polymerase chain reaction (PCR) in CSF was positive for EBV DNA (250 EBV copies/mL, on the day of admittance). Plasma EBV PCR was also positive, with a rising number of copies throughout the inpatient stay (79 EBV copies/mL, two days after admission; 315 EBV copies/mL, 12 days after admission). EBV plasma serology performed two and 12 days after admission showed, on both occasions, positive anti-EBV viral capsid antigen (VCA) IgG, negative anti-EBV VCA IgM, and positive anti-EBV nuclear antigen (EBNA) IgG.
A multiplex PCR CSF meningoencephalitis panel and CSF culture were negative (Table 1). Mycoplasma pneumonia plasma serology was IgM positive and IgG negative. Mycoplasma pneumonia PCR in CSF was negative. Cytomegalovirus (CMV) plasma serology was IgG positive and IgM negative. HIV serology was negative. The remaining plasma serologies and a nasopharyngeal multiplex PCR panel were negative (Table 1).
An autoimmunity plasma screen was positive for antinuclear antibodies (ANA) with an anti-nucleolar homogeneous pattern (AC-8, titer of 1:160). Plasma antiganglioside antibodies (AGA) were IgM weakly positive for GM3 and GQ1b and IgG negative. Rheumatoid factor and anti-cardiolipin IgG and IgM antibodies were not detected (Table 1).
On the second day after admission the EEG showed diffuse brain dysfunction with no epileptic activity. The patient was uneventfully extubated. She had a gradual clinical improvement, with no seizures observed since extubation. Fever resolved by day two of admittance and no further episodes of vomiting were noted since admission.
The patient developed post dural puncture headache, which resolved by the fifth day after admission. On the fourth day after admission, blood analysis showed hepatic cytolysis and cholestasis (increased serum transaminases, alkaline phosphatase and gamma-glutamyl transpeptidase), requiring a switch from ceftriaxone to cefotaxime. Subsequently, there was a gradual analytical improvement with no other complications observed during the inpatient stay.
Cefotaxime was discontinued after negative cultural results. A presumptive diagnosis of EBV viral encephalitis was made and treatment with acyclovir was maintained for 14 days. Blood counts and CRP were within normal values prior to discharge. The last EEG, performed on day 10 of admittance, presented a slight improvement since admission, compatible with mild diffuse brain dysfunction.
The patient was discharged home seizure-free, 12 days after admission, on levetiracetam. On a follow-up appointment at nine months post-discharge, she had a normal brain MRI as well as an EEG with normal background activity and no epileptiform discharges, having recovered her premorbid function in activity and school performance. In this appointment, levetiracetam started to be weaned off. | | | | Discussion | Encephalitis is defined as inflammation of the brain parenchyma and can be caused by infection or autoimmunity.1 The most common etiology is viral and is most frequently due to infection by HSV-1 and HSV-2, non-polio enteroviruses, and arboviruses.1 EBV is also a causative agent and can affect immunocompetent individuals.2 The prevalence of EBV encephalitis/meningoencephalitis ranges across studies, from 2 to 31%.3
EBV is usually associated with infectious mononucleosis (IM), a disease most commonly affecting teenagers, which presents with fever, pharyngitis, headache, lymphadenopathy, splenomegaly, and leukocytosis with atypical lymphocytes.4 In young children most primary EBV infections are asymptomatic, although they can also lead to various neurological complications, such as encephalitis or meningitis.4 The clinical presentation of EBV encephalitis tends to be nonspecific and has been associated with a prodrome of fever and headache instead of the constellation of infectious mononucleosis symptoms.3,5 This may be due to the pathogenesis of EBV related-CNS diseases, which can be associated with latent viral reactivation or an antibody-mediated post-inflammatory response, possibly leading to a clinical picture that is different from IM.3 We should thus consider EBV as one of the causative agents of acute encephalitis in young children, regardless of presenting symptoms or immune status.
In our patient, the prodrome of fever, headache and vomiting followed by tonic-clonic seizures evolving to status epilepticus associated with the plasma, CSF, neuroimaging, and EEG findings reported are consistent with an acute viral encephalitis. She had positive EBV PCR in CSF and increasing EBV copies in plasma PCR during her inpatient stay, which is now preferred as a diagnostic tool over viral culture or serological diagnosis.6 On the other hand, she had a positive plasma serology for anti-EBV VCA IgG and anti-EBNA and a negative plasma serology for anti-EBV VCA IgM. These findings may be associated with an EBV reactivation, which has been reported both in immunocompetent and immunodeficient patients.7 It is, however, debatable whether positive EBV DNA in CSF detected by quantitative PCR indicates active lytic infection versus only latent genome, as EBV may be subclinically reactivated due to other pathological CNS conditions.7,8 As a limitation to our case, we did not perform CSF or plasma anti-EBV early antigen (EA) serology, which could have helped in establishing a diagnosis of EBV reactivation in our patient, as it rises with primary infection and reactivation.9 Moreover, we did not calculate the EBV-antibody index in the CSF, which could have helped to elucidate pathophysiology, namely the extent to which a possible immune response might be at play in her condition.10
Other infectious causes were largely excluded by multiplex PCR CSF and nasopharyngeal panels, CSF culture, as well as serological plasma testing. The positive IgM Mycoplasma pneumonia plasma serology could point to an acute infection caused by this pathogen but was more likely due to cross-reactivity with an acute EBV infection or to the low-specificity associated with this test.11 This hypothesis is also supported by the negativity of Mycoplasma pneumonia PCR in CSF.
We did not perform CSF testing for autoimmune etiologies as clinical suspicion was low for autoimmune encephalitis (AE). Nonetheless, it is of note that anti-N-methyl-D-aspartate receptor (anti-NMDAR) encephalitis, the most common form of antibody-mediated AE, can often begin with a viral prodrome, which may consist of fever, headache, and gastrointestinal symptoms, as seen in our patient.12 After the prodrome, initial manifestations of disease, especially in young children, often include neurological symptoms, such as seizures, as opposed to predominantly psychiatric symptoms, as is commonly seen in adults. However, irrespective of initial presentation, 90% of children will progress to at least three symptoms, including psychiatric features, memory disturbance, seizures, dyskinesias, change in the level of consciousness or autonomic dysfunction, in the first month after onset.12 This did not occur in our patient, who recovered to premorbid status less than three months after presentation. Anti-NMDAR encephalitis has been linked to EBV reactivation, in a case report where this diagnosis was concurrent with positive CSF anti-EBV EA IgG in three patients.13 All the patients in the report presented with both psychiatric and neurologic symptoms, and EBV encephalitis was unconfirmed due to the lack of EBV PCR in CSF. We did not perform CSF anti-EBV EA serologies but did find a positive EBV PCR in CSF, as discussed above.
The incidence of AGAs has not been sufficiently studied in healthy individuals, but appears to range from 1 to 9% in healthy control groups in AGA studies.14 Of potential interest for follow-up, anti-GM3 and anti-GQ1b AGAs, which in our patient were IgM weakly positive, have both been associated with primary multiple sclerosis, among other diseases.14 Anti-GQ1b AGA has also been linked to Guillain-Barré Syndrome (GBS), and GBS to previous EBV and other infections, although this has not yet been confirmed in the pediatric population.15,16 Also of note, decreased immune control of chronic EBV infection has been found to contribute to the development of Systemic Lupus Erythematosus, which could be relevant in our patient as she had a positive ANA.17
Brain MRI showed mainly focal cortical involvement, which has previously been associated with a good prognosis.18 Bilateral T2 hyperintense lesions of the basal ganglia and thalami have been associated with EBV encephalitis but were not present in our patient.19 EEG changes in viral encephalitis are usually nonspecific and have been reported to include generalized or focal brain disfunction, epileptiform discharges, status epilepticus and FIRDA, some of which were present in our patient.4,20
There are currently no standard guidelines for the treatment of EBV encephalitis, though many authors opt for a therapeutic cycle of 14 to 21 days of acyclovir or ganciclovir.3,21 Corticosteroids may be beneficial in the setting of immune-mediated EBV-associated neurologic involvement. The prognosis of EBV encephalitis tends to be good, as was the case for our patient at nine months’ follow-up.20 EBV encephalitis-associated status epilepticus has, however, been reported to be associated with a worse prognosis, including prolonged intensive care stay and death.4,22,23
In conclusion, EBV encephalitis should be considered in any child who presents with possible viral encephalitis features. Its diagnosis remains challenging and should be guided by clinical manifestations, laboratory, CSF, neuroimaging, and EEG findings. CSF PCR is the preferred method for establishing the diagnosis. Treatment with antiviral agents is generally recommended and prognosis is good overall.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Costa BK da, Sato DK. Viral encephalitis: a practical review on diagnostic approach and treatment. J Pediatr (Rio J). 2020;96(Suppl 1):12. doi:10.1016/J.JPED.2019.07.006. [CrossRef]
- Carneiro VC de S, Pereira JG, de Paula VS. Family Herpesviridae and neuroinfections: current status and research in progress. Mem Inst Oswaldo Cruz. 2022;117. doi:10.1590/0074-02760220200. [CrossRef]
- Pangprasertkul S, Sanguansermsri C, Sudjaritruk T. Epstein-Barr virus meningoencephalitis in a young immunocompetent child: A case report. Heliyon. 2022;8(10):e11150. doi:10.1016/J.HELIYON.2022.E11150. [CrossRef]
- Doja A, Bitnun A, Ford Jones EL, et al. Pediatric Epstein-Barr virus-associated encephalitis: 10-year review. J Child Neurol. 2006;21(5):384-391. doi:10.1177/08830738060210051101. [CrossRef]
- Kneen R, Michael BD, Menson E, et al. Management of suspected viral encephalitis in children - Association of British Neurologists and British Paediatric Allergy, Immunology and Infection Group National Guidelines. Journal of Infection. 2012;64(5):449-477. doi:10.1016/J.JINF.2011.11.013/ATTACHMENT/E7F1BBFE-3A0E-4902-A652-CFBC8C2FE927/MMC2.PDF. [CrossRef]
- Autore G, Bernardi L, Perrone S, et al. Update on Viral Infections Involving the Central Nervous System in Pediatric Patients. Children (Basel). 2021;8(9). doi:10.3390/CHILDREN8090782. [CrossRef]
- Sanefuji M, Ohga S, Kira R, et al. Epstein-Barr virus-associated meningoencephalomyelitis: intrathecal reactivation of the virus in an immunocompetent child. J Child Neurol. 2008;23(9):1072-1077. doi:10.1177/0883073808315414. [CrossRef]
- Sundén B, Larsson M, Falkeborn T, et al. Real-time PCR detection of human herpesvirus 1-5 in patients lacking clinical signs of a viral CNS infection. BMC Infect Dis. 2011;11. doi:10.1186/1471-2334-11-220. [CrossRef]
- Gulley ML. Molecular diagnosis of Epstein-Barr virus-related diseases. J Mol Diagn. 2001;3(1):1-10. doi:10.1016/S1525-1578(10)60642-3. [CrossRef]
- Kleines M, Schiefer J, Stienen A, et al. Expanding the spectrum of neurological disease associated with Epstein-Barr virus activity. European Journal of Clinical Microbiology and Infectious Diseases. 2011;30(12):1561-1569. doi:10.1007/S10096-011-1261-7/METRICS. [CrossRef]
- MacDonald B, Diamond Y, McCloskey K, et al. Probable acute Epstein-Barr virus encephalitis in a 6-year-old girl. J Paediatr Child Health. 2017;53(12):1233-1235. doi:10.1111/JPC.13642. [CrossRef]
- Hardy D. Autoimmune Encephalitis in Children. Pediatr Neurol. 2022;132:56-66. doi:10.1016/J.PEDIATRNEUROL.2022.05.004. [CrossRef]
- Hou R, Wu J, He D, et al. Anti-N-methyl-D-aspartate receptor encephalitis associated with reactivated Epstein-Barr virus infection in pediatric patients: Three case reports. Medicine. 2019;98(20). doi:10.1097/MD.0000000000015726. [CrossRef]
- Cutillo G, Saariaho AH, Meri S. Physiology of gangliosides and the role of antiganglioside antibodies in human diseases. Cellular & Molecular Immunology 2020 17:4. 2020;17(4):313-322. doi:10.1038/s41423-020-0388-9. [CrossRef]
- Rodríguez Y, Rojas M, Pacheco Y, et al. Guillain-Barré syndrome, transverse myelitis and infectious diseases. Cell Mol Immunol. 2018;15(6):547-562. doi:10.1038/CMI.2017.142. [CrossRef]
- Lubarski K, Mania A, Michalak S, et al. The Clinical Spectrum of Autoimmune-Mediated Neurological Diseases in Paediatric Population. Brain Sci. 2022;12(5). doi:10.3390/BRAINSCI12050584. [CrossRef]
- Houen G, Trier NH. Epstein-Barr Virus and Systemic Autoimmune Diseases. Front Immunol. 2021;11. doi:10.3389/FIMMU.2020.587380. [CrossRef]
- Abul-Kasim K, Palm L, Maly P, et al. The neuroanatomic localization of Epstein-Barr virus encephalitis may be a predictive factor for its clinical outcome: a case report and review of 100 cases in 28 reports. J Child Neurol. 2009;24(6):720-726. doi:10.1177/0883073808327842. [CrossRef]
- Yang CWR, Mason M, Parizel PM, et al. Magnetic resonance imaging patterns of paediatric brain infections: a pictorial review based on the Western Australian experience. doi:10.1186/s13244-022-01298-1. [CrossRef]
- Cheng H, Chen D, Peng X, et al. Clinical characteristics of Epstein-Barr virus infection in the pediatric nervous system. BMC Infect Dis. 2020;20(1). doi:10.1186/S12879-020-05623-1. [CrossRef]
- Matthews E, Beckham JD, Piquet AL, et al. Herpesvirus-Associated Encephalitis: an Update. Curr Trop Med Rep. 2022;9(3):92-100. doi:10.1007/S40475-022-00255-8. [CrossRef]
- Rodrigo-Armenteros P, Kapetanovic-García S, Antón-Méndez L, et al. Akinetic mutism and status epilepticus due to Epstein Barr virus encephalitis. Clin Neurol Neurosurg. 2019;185:105492. doi:10.1016/J.CLINEURO.2019.105492. [CrossRef]
- Mathew AG, Parvez Y. Fulminant Epstein Barr virus encephalitis. Indian Pediatr. 2013;50(4):418-419. doi:10.1007/S13312-013-0101-5. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2026.68
|
| Cite this article as: | | Salvada A, Silva M F, Mota A F, Costa F, Rocha S, Cruz L R, Correia P, Luís C. Probable Epstein-Barr virus encephalitis presenting with status epilepticus in an 8-year-old. Pediatr Oncall J. 2024 Aug 30. doi: 10.7199/ped.oncall.2026.68 |
|