Introduction
ASD is a congenital heart defect (CHD). CHDs are very common in children, 8 per thousand is the prevalence. ASD contributes about 15-20% of CHDs. Interatrial communication i.e Patent Foramen Ovale(PFO) is essential for fetal survival hence Fossa ovalis ASD is difficult to rule out antenatally. Although fetal echo can rule out ASD by the absence of flap of the fossa ovalis.
PFO may remain patient in 25% after delivery.
Embryology:- (classic model) & type of ASD
A crescent-shaped septum (septum primum) begins to form along the dorsal and cranial wall of the primitive atrium and grows towards the endocardial cushions. Then small perforations develop in the dorsal wall of the septum to form ostium primum. If the endocardial cushions fail to unite to septum primum then the ostium primum type of ASD is formed.
Then septum Secundum migrates from right side of the septum to close the ostium primum. Failure of migration of the septum secondum or excess resorption of septum primum dorsally forms fossa ovalis ASD.
The sinus venosum unites with the primitive atrium from the right side to form RA. Failure to unite results in sinus venous type of ASD (IVC, SVC, atrial type).
Atrial Septic Defect - Presentation
II PRESENTATIONS:
Normally, blood flows from RA? RV? PA? PV? LA? LV? AO? IVC/SVC? RA. In ASD blood shunts from LA? RA because of higher LA pressure, Then RA, RV becomes overloaded over a period of 1 to 4 years. RA? LA shunt will only occur if there is Tricuspid atresia/PAH/TAPVC. The bidirectional shunt will occur in (transposition of great vessels)TGA. In ASD with MS, RA, RV volume overload comes earlier. Note:- As ASD is a low-pressure shunt unlike VSD, the clinical features appear late.
AGE:
Usually, symptoms appear in late childhood (>4 years) or adolescence. In large ASD, symptoms have been seen at 1 year of age also. ASD is the most common CHD in adults.
SEX:
F:M = 2:1
Clinical Features And Investigations
Clinical Features:
- Incidental findings: Many children with ASD are detected on routine examination-- systolic murmur in a pulmonary area or wide fixed split of S3.
- Failure to thrive - may be seen in large ASDs.
- Dyspnea on exertion may be present after 4 years of age.
- Arrhythmias - adults may present with arrhythmias.
- Recurrent LRTI? may be seen with a large ASD.
Physical findings:
Inspection: Precordial buldge and increased precordial activity may be seen.
Palpitation: Parasternal heave s/o RV volume overload, cardiac enlargement, a shift of apex to down & out.
Auscultation: Prominent P2 s/o PAH, wide fixed split, ejection systolic murmur in pulmonary area s/o increased flow across PV, mid-diastolic murmur in tricuspid area s/o underflow across the TV.
III. Investigations:
CXR:- cardiomegaly (Right atrial enlargement + Right ventricular enlargement)
RAE? >extending upto 3 ribs on right parasternal area.
RVE? Apex down and out
Increased pulmonary vascular markings.
Figure 1 : Chest x ray ap view I a case of ASD showing dilated right atrium and right ventricle with increased blood flow to the pulmonary vascular bed

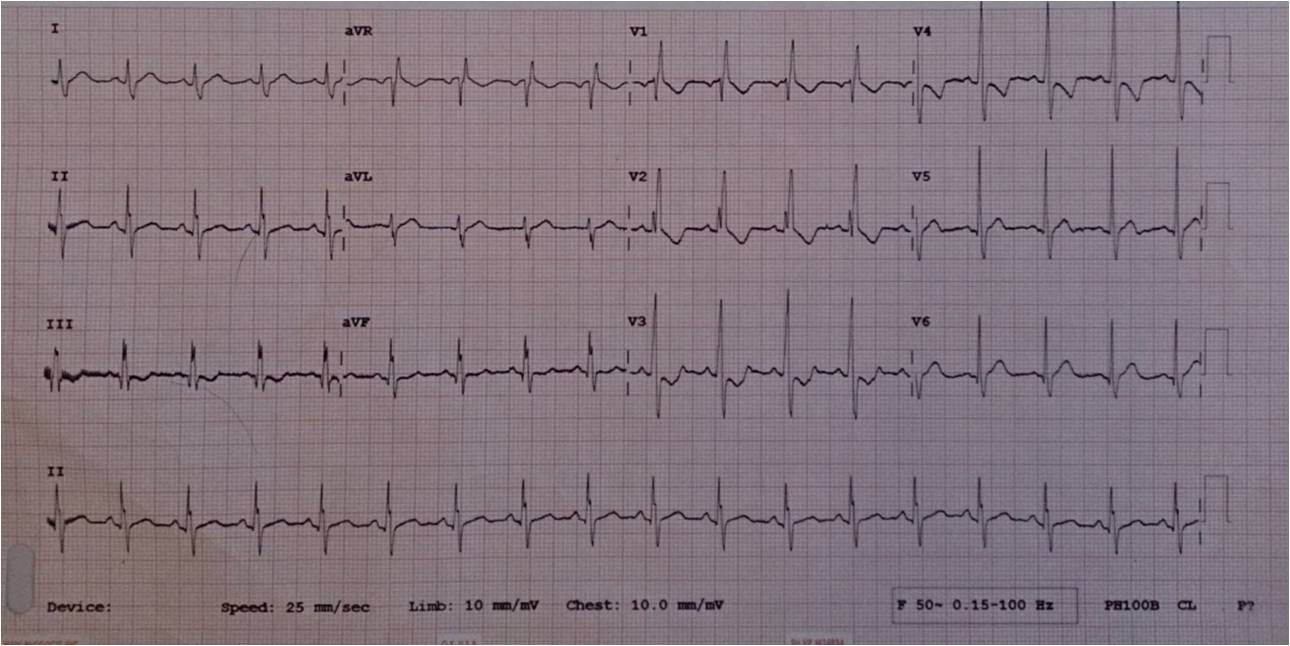
ECG:
Pathognomic of RV Volume Overload
Figure 2 : electrocardiogram in a case of ASD showing features of right sided dilatation. Note the presence of partial RBBB and crochette sign.
ECHO:-
Echo is an essential modality to delineate the ASD and its types. Diagnosis confirmed on the subcostal view. Echo is essential to look at the site of ASD, to looks for the rims of ASD (to ascertain for suitability for the device closure of ASD), to look for associated features of ASD, to look for the evidence of pulmonary artery hypertension. To look for associated anomalies.
Figure 3 : Echocardiography image in subcoastal view showing the fossa ovalis ASD with atrial rim ( marked by arrow) and AV rim ( marked by star)
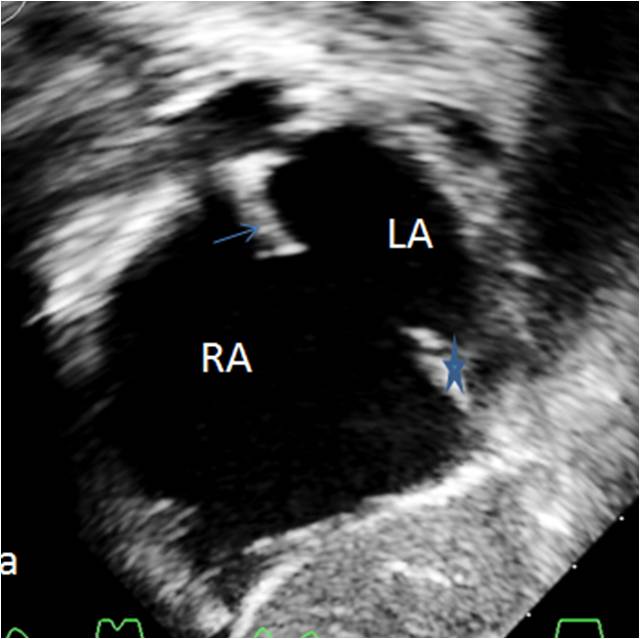
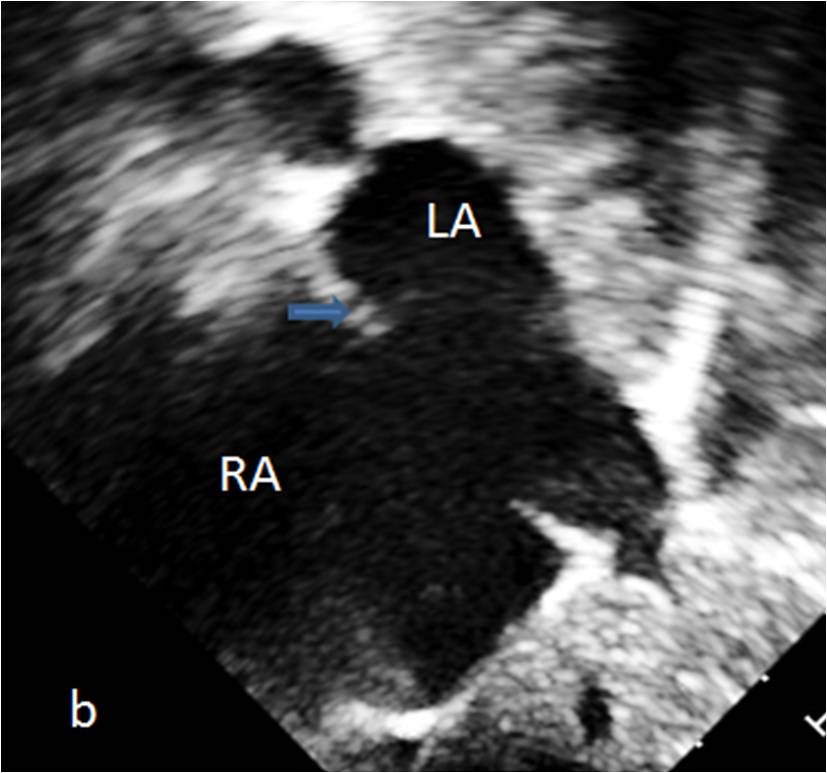
Figure 3a: Echocardiography image in subcoastal view showing the fossa ovalis ASD with SVCl rim ( marked by arrow) and deficient IVC rim . Such ASD are not considered suitable for ASD device closure
Transesophageal echocardiography (TEE):-
Usually required in adults in view of the poor subcostal windows and during device closure in children too.
Cath:
Usually required in adults to r/o under PVR & also during device closure.
RA, RV, PA, PV, LV, Ao pressures and saturations are taken pulmonary vascular resistance is calculated as= PA-PV pressure/Pulmonary flow(Qp), and Qp= O2 consumption/Hbx10x(PV-PA SpO2).PVR up to 8 kinds of wood unit non-modifiable on O2 is accepted as treatable.
Angiography may be done to rule out any associated CHDs like PAPVC, PV anomaly.
BNP Levels:
May be elevated in CHF/volume overload.
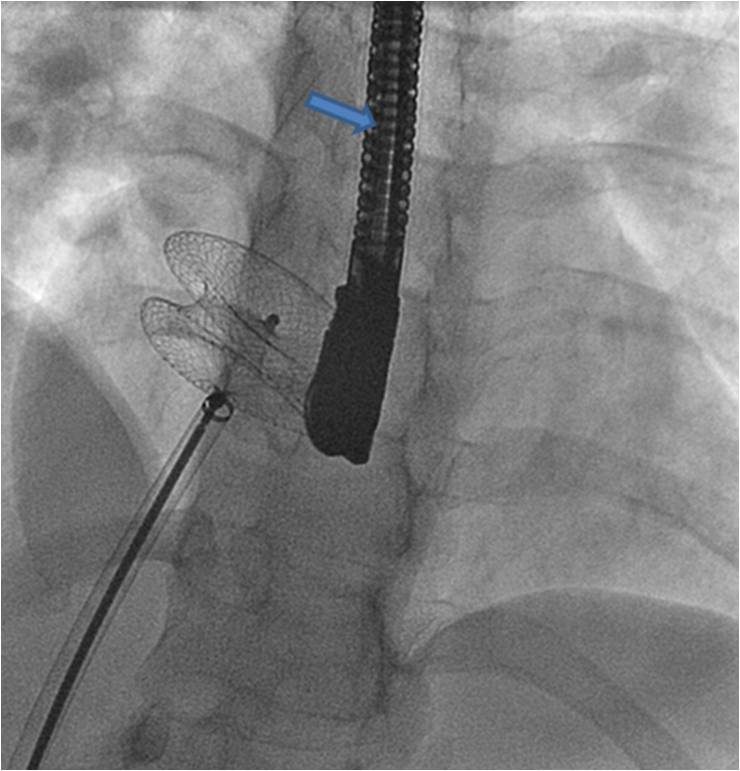
Figure 4 : Flouroscopy image of the case of ASD , undergoing a ASD device closure in LAO carnail View ( 30/30 degree) showing the ASD device ins situ. Also note the prescence of TEE probe ( marked by arrow).
Treatment
Management And Natural History of Treated and Untreated ASD
TREATMENT:
Medial:
Antifailure treatment in the form of diuretics is very rarely required. These may be given if there is evidence of congestive heart failure. Antiamythics may be given in adults >40 years if there are associated arrhythmias.IE prophylaxis is not recommended.
Spontaneous closure.
Is seen in ASD <4 mm before 4 years of life.
Surgical closure:-
Indications:
If device closure not possible because of deficient rims then only surgical closure is recommended.
Ideal age of closure: (IAP guidelines)
- In asymptomatic child (2-4 years) class I (for SV ASD surgery may be delayed 4-5 years class IIa).
- Symptomatic ASD in infancy (CHF, severe PAH) seen in 10% cases. Rule out TAPVC, APW, LVOTO- early closure is recommended (class I)).
- If presenting beyond ideal age; elective closure irrespective of age as long as there is RV overload and PVR is inoperable range (class I).
DEVICE CLOSURE:
ASD occluders are available up to 40 mm for device closure.
Atrial, aortic, SVC, and IVC rims should be at least 5 mm so that the device can sit properly.
The device is made of nitinol wire (nickel & titanium) and Dacron meshwork embedded on it.
The device is advanced under fluoroscopic guidance from IVC? RA? ASD? LA and released across the IAS with the delivery catheter under TEE guidance.
Complication:
- Device embolisation may occur in to RA, RV/PV if it does not sit properly or if rims are not good. In that case it may be snared back under flouro. Usually surgery is required, so CTVS background is must.
- Very rarely 1; 1000 it may erode into aortic root.
Surgical closure:
Dacron patch closure of ASD is done under CPB with good results.
Complications:
- General complications of surgery and CPB.
- Residual shunt.
Longterm complications (Natural history)
Mean age to death = 37.5 + 4.5 years, 75% die by 50 years, 90% die by 60 years of age.
Spontaneous closure (mean follow up of 14 months).
<3 mm - generally all close.
3-5 mm - 87% close
5-8 mm - 80% close
>8 mm - generally none
The pulmonary vascular obstructive disease develops in patients with large left to right shunt. In a young adult, there is a 14% chance of developing PAH.
Arrhythmias - atrial flutter and fibrillation develops in 1% cases <40 years of age, 40 to 60 years 15% develops arrhythmias, >60 years 61% develops arrhythmias.
1. Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol 2002, 39:1890-1900.
2. Mainwaring RD, Mirali-Akbar et.al. Secundum type atrial septal defects with failure to thrive in the first year of life. J Card Surg 1996;11:116-120.
3. Morgan GJ, Casey F et.al. Assessing ASDs prior to device closure.
4. Teo KS, Disney PJ. Assessment of ASD comparing cardivasular magnetic resonance with TEE. J Cardiovasc Magn REson 2010;12:44.
5. Campbell M, Natural history of ASD. Br Heart J 1970;32:820-826.
6. Babic UU et.al. double umbrella device for trans venous closure of PD and ASD colon first experience. J INterv Cardiol 1991;4:283-294.
7. Indian pediatric 2008;45:117-126.