Associated Anomalies with Congenital Heart Disease
Musculoskeletal - 8.8%
Specific Syndromes - 8.5%
Central Nervous - 6.9%
Urinary - 5.3%
Gastrointestinal - 4.2%
Respiratory - 3.8%
Endocrine - 1.3%
Immunologic-Hematologic - <1.0%
Reproductive - <1.0%
Other 2.9%
Recurrence Risks Given One Sibling Who Had a Cardiovascular Anomaly
VSD - 3%
PDA - 3%
ASD - 2.5%
TF - 2.5%
PS - 2%
CoA - 2%
AS - 2%
D-TGA - 2%
AV Canal- 2%
EFE - 4%
TA - 1%
Ebstein's Anomaly - 1%
Truncus Arteriosus - 1%
PA - 1%
HLHS - 2%
Congenital Heart Disease - Definition
Congenital heart disease is defined as the structural, functional or positional defect of the heart in isolation or in combination, present from birth, but may manifest at any time after birth or may not manifest at all.
Congenital heart disease remains a problem of major importance particularly for the family physician, who is first in the line of medical professionals, to diagnose and counsel the patients and the family. It is the most common single group of congenital abnormalities accounting for about 30 percent of the total.
Congenital Heart Disease - Incidence
The general reported incidence varies from 8-10 per 1000 live newborn population. There are eight common lesions, which account for 85 percent of all cases. They are:
- ventricular septal defect (VSD)
- patent ductus arteriosus (PDA)
- atrial septal defect (ASD)
- pulmonary valve stenosis
- aortic valve stenosis
- coarctation of the aorta
- Tetralogy of Fallot
- Transposition of great arteries
The remaining 15 percent accounts for a variety of more rare and complex lesions. Congenital heart disease as a whole occurs with an equal frequency in males and females but some lesions such as aortic stenosis, coarctation of the aorta are more common in males, while patent ductus arteriosus and atrial septal defects are more common in females. About 13 percent of patients with one heart defect, will have an additional cardiac defect. About 10 to 15 percent of patients with heart defects will have another non-cardiac deformity. The risk of siblings being affected by congenital heart disease is between 2 and 4 percent. So, parents who have had one child with congenital heart disease should, if they wish, be advised by a genetic counselor.
Congenital Heart Disease - Etiology
No specific causes are found in most cases of congenital malformations of the heart. In minority cases, clear-cut single causes, either environmental or genetic, are responsible. No good evidence is available implicating the interaction of specific genetic and exogenous factors in the causation of cardiac malformation in man, though experiments on animals suggest such an interaction.
Inheritance
A few families are reported in which defect follows dominant pattern of inheritance, e.g. atrial septal defect, supravalvular aortic stenosis, cardiomyopathy. Recessive autosomal inheritance confined to the heart is exceptional.
Chromosomal Abnormalities
About 5 percent of patients with congenital heart disease are associated with some chromosomal abnormalities (Table 1).
Table 1: Incidence of Congenital Heart Disease with chromosomal abnormalities
| Chromosome abnormality |
Name of syndrome |
Incidence of CHD (percentage) |
Type of defect |
| 21 Trisomy |
Down's syndrome |
60 |
A-V canal defect VSD |
| 18 Trisomy |
- |
90 |
VSD, PDA, DORV |
| 13 Trisomy |
- |
90 |
Dextrocardia, VSD, PDA |
| XO |
Turner's syndrome |
15 |
Coarctation of aorta, aortic stenosis |
Environmental Factors
Increased incidence of congenital heart defect has been noted with intrauterine viral infections, maternal drug consumption during the first trimester of pregnancy, and pregnancy-induced systemic maternal diseases. (Table 2)
Table 2: Incidence of Congenital Heart Disease with environmental factors.
Maternal Infections:
- Rubella: PDA, pulmonary stenosis, VSD, ASD
- Mumps: Endocardial Fibroelastosis
Maternal Drugs
- Phenytoin: Variable
- Vitamin D: Supravalvular aortic stenosis
Maternal Disease
- Diabetes: Transposition of great arteries
- Systemic Lupus Erythematosus: Congenital Heart Block
Multifactorial Causation
The most accepted theory for the genetic basis of congenital heart disease is a multifactorial hypothesis. It suggests that the abnormalities of genes may not be enough to cause cardiac malformations, but may manifest in the presence of above mentioned adverse environmental hazards.
Congenital Heart Disease - Classification
Congenital heart diseases are basically divided into the following groups:
- Structural heart defects
- Functional heart defects, e.g. congenital cardiac arrhythmias
- Positional heart defects, e.g. dextrocardia
Structural heart defects are divided into two main groups:
- Acyanotic defects
- Cyanotic defects
Each group is subdivided according to:
- pulmonary blood flow: increased, decreased or normal
- dominant ventricle - left or right
- pulmonary hypertension - present or absent
The clinical diagnosis of a congenital heart is complex when first considered but with sound anatomy and physiologic principles and proper understanding of clinical manifestations, it may become simple. If information is handled with the framework of the following figures, the clinical diagnosis becomes simple.
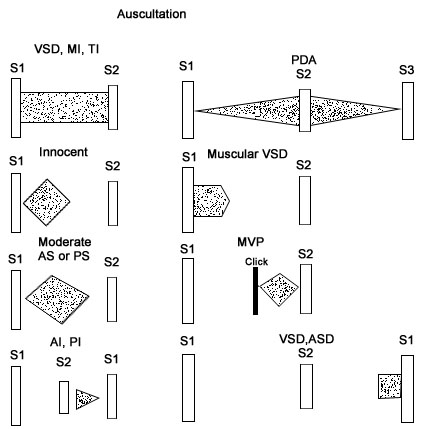
Murmurs
- Incidence: 2/3 to 3/4 of all children
- Types of murmurs: systolic, diastolic and continuous
- Groups of murmurs:
- Functional murmur - secondary to anemia, fever etc.
- Innocent murmur - Still's murmur, venous, hum, etc
- Organic murmur - secondary to cardiovascular defect function
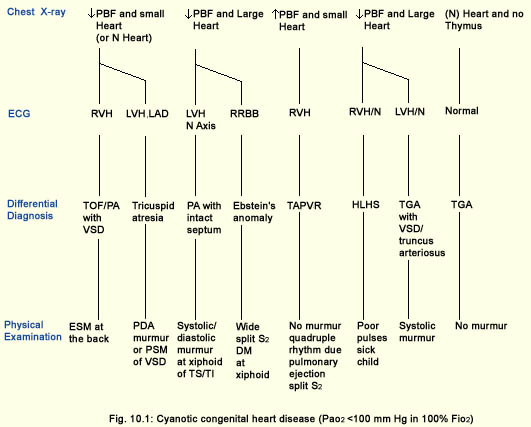
Cyanosis
Causes of cyanosis with excessive pulmonary blood flow:
- Transposition of great arteries
- Total anomalous pulmonary venous return
- Hypoplastic left heart syndrome
- Truncus arteriosus
Causes of Cyanosis with Inadequate Pulmonary Blood flow
- Pulmonary atresia or severe stenosis with
- Ventricular septal defect
- Intact ventricular septum
- Tricuspid atresia or stenosis
- Tricuspid insufficiency
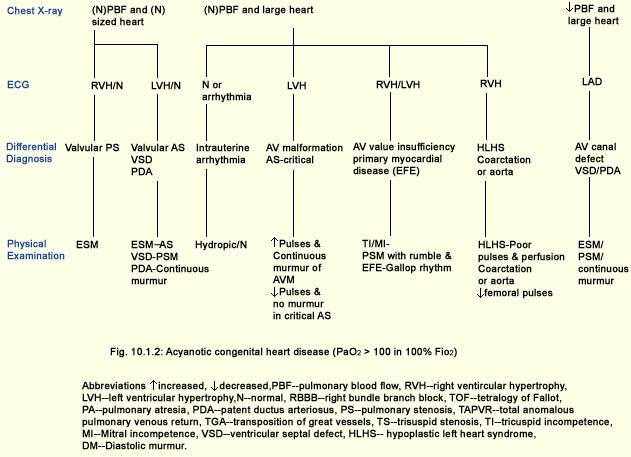
Congestive Heart Failure
Causes of CCF in 1st week of life:
Cardiac causes:
- Hypoplastic left heart syndrome
- Coarctation of aorta
- D-transposition of great arteries
- Myocarditis
Extracardiac causes:
- A-V malformation
- Anemia
- Polycythemia
- Infant of diabetic mother
Causes of CCF after 1st week of life
In a 2 month old:
- D-transposition of great arteries
Between 2 months to 6 months of age:
- Ventricular septal defect
- Patent ductus arteriosus
- Endocardial cushion defect
- Endocardial fibroelastosis
- Anomalous left coronary artery
- Left ventricle obstruction
Between 6 months to 1 year of age:
- Endocardial fibroelastosis
- Ventricular septal defect
Between 1 year to 15 years of age:
- Myocarditis
- Rheumatic fever
- Subacute bacterial endocarditis
- Acute glomerulonephritis
Congenital Heart Disease - Clinical Presentation
Despite a large number of cardiac defects that exist, there are only a limited number of physiological disturbances that can be produced. Congenital heart disease usually presents in infancy as cyanosis or heart failure or a combination of both, heart murmur, circulatory shock, stridor, hypercyanotic spells, different respiratory tract infections, and growth failure.
Cyanosis
Cyanosis is blue discoloration of the skin, mucus membranes, and nails due to the presence of desaturated hemoglobin more than 5 gm/dl percent in arterial blood. Those cardiac anomalies in which systemic venous return reaches systemic circulation without passage through the lungs, presents with central cyanosis and clubbing of fingers.
Cyanosis occurs under following circumstances:
- Reduced pulmonary blood flow in defects with right ventricular outflow tract obstruction
- Right to left shunts as in Tetralogy of Fallot
- Discordant ventriculoarterial connections as in transposition of great arteries, and
- Mixing of venous and arterial blood as in truncus arteriosus or single ventricle.
Heart Failure
When the heart cannot supply the blood flow demanded by tissues, a clinical syndrome of symptoms and signs manifest from elevated atrial pressure. It manifests with rapid and labored breathing due to pulmonary edema, pallor with peripheral cyanosis due to poor cardiac output, tachycardia, and excessive sweating due to increased sympathetic activity and feeding difficulties.
Heart failure occurs in following situations:
- Volume overload in all defects with left to right shunt like ventricular septal defect, atrial septal defect, patent ductus arteriosus,
- Pressure overload in pulmonary and aortic valve stenosis
- Intrinsic myocardial diseases as in cardiomyopathies, and
- Decreased or increased diastolic fillings as in tachyarrhythmias and bradyarrhythmias.
Heart Murmurs
In older children and in infants, congenital heart disease presents as a heart murmur detected on routine examination. The murmurs are produced due to abnormal pressure gradient across laminar or nonlaminar pathways. The murmur is continuous in patent ductus arteriosus, pansystolic in ventricular septal defect and pulmonary stenosis, and diastolic in atrioventricular valve stenosis.
Shock
Cardiac malformations resulting in a hypoplastic ascending aorta, aortic atresia result in low cardiac output. The child appears extremely ill with cold extremities, diminished pulses, low blood pressure, peripheral cyanosis, and is semicomatose.
Hypercyanotic Spells
In cardiac malformations with pulmonary infundibular stenosis, the obstruction is of dynamic variety. Whenever the muscular outflow tract contracts, blood flow to the pulmonary circuit diminishes and the patient gets intense cyanosis. It occurs in Fallot's tetralogy and defects with Fallot's physiology.
Stridor
Malformations leading to compression of trachea and bronchi causing obstruction of the airways, present with stridor, as seen in vascular rings and in a dilated pulmonary artery due to increased pulmonary blood flow.
Chest Pain
Malformations like the anomalous origin of the left coronary artery, severe aortic stenosis lead to myocardial ischemia and the patient presents with episodes of screaming, pallor, and chest pain.
Recurrent Respiratory Tract Infections
In cardiac defects with a left to right shunt, as seen with a ventricular septal defect and patent ductus arteriosus, there is a decreased lung compliance which leads to frequent respiratory tract infections.
Growth Failure
Growth failure is a very common manifestation of heart defects due to poor oxygen saturation in the growing tissues, persistent heart failure, and frequent respiratory infections with undernutrition.
1. Park M: Pediatric Cardiology for the Practitioner.
2. Adams FH, Emmanouilides GC (eds): Heart Disease in Infants, Children and Adolescents. Williams & Wilkins, Baltimore/London, 1983.
3. Rudolph AM (Ed), Hoffman J (co Ed): Pediatrics, Appleton-Century-Crofts, Norwalk, Conn., 1977.Abbreviations:
4. VSD - Ventricular septal defect.
5. PS - Pulmonary stenosis.
6. PDA- Patent ductus arteriosus.
7. TOF - Tetralogy of fallot.
8. AS - Aortic stenosis.
9. ASD - Atrial septal defect.
10. CoA - Coarctation of aorta.
11. D-TGA - D-Transposition of great arteries.
12. ECD - Endocardium cushion defect.
13. A-V Canal - Atrioventricular canal.
14. AI - Aortic insufficiency.
15. MVP - Mitral valve prolapse.
16. PPS - Peripheral pulmonary stenosis.
17. HLHS - Hypoplastic left heart syndrome.
18. TAPVR - Total anomalous pulmonary venous return.
19. EFE - Endocardium fibroelastosis.
20. LV obst. - Left ventricular obstruction.
21. Anomalous L. Cor. Art. - Anomalous left coronary artery.
22. SBE - Subacute bacterial endocarditis.
23. AGN - Acute glomerulonephritis.
24. TA - Tricuspid atresia.
25. PA - Pulmonary atresia.
26. LLSB - Left lower sternal border.
27. LUSB - Left upper sternal border.
28. RUSB - Right upper sternal border.
29. RVH - Right ventricular hypertrophy.
30. LVH - Left ventricular hypertrophy.
31. RAD - Right axis deviation.
32. RAE - Right atrial enlargement.
33. LAE - Left atrial enlargement.
34. BVH - Biventricular hypertrophy.
35. PVOD - Pulmonary vascular obstructive disease.
36. Tx - Treatment.
37. HS - Heart size.
38. PV - Pulmonary vascularity.
39. MPA - Main pulmonary artery.