Introduction
the first case with truncus arteriosus was reported by Wilson in 1798, and the existence of the entity was confirmed by accurate clinical and autopsy reports of a 6-month-old infant by Buchanan in 1864.
Morphogenises And Genetics
The actual cause of the embryological disturbance that results in the development of truncus arteriosus lesions is not known.
Most of the early embryological studies suggesting the association between the number of migrated neural crest to the aortopulmonary outflow.
Monoallelic microdeletion of chromosome 22q11 (DiGeorge syndrome) is identified in up to 40% of patients with truncus arteriosus
Anatomy
- large common outflow trunk for right and left sides of the heart with single valve.
- Truncal Valve: can vary from bicuspid leaflet valve up to 7 leaflets in the valve. the communist anatomy is the trileaflet valve.
- Pulmonary arteries vary in position (more details in classification)
- The ventricular septal defect; almost always present at sub-arterial position.
- Coronary ostium position anomalies in not unusual especially the left ostium near by the pulmonary arteries takeoff or with right ostium.
Natural History
The lesion is rapidly lethal in most patients, with a median
survival times being about 5 weeks to 5 months, less than 20% survive more than a year, and less than 5% more than 5 years except in the series reported by Collett and Edward and by Fontana and Edwards
Truncus Arteriosus - Definition
This condition defined as the presence of a single semilunar valve and annulus with a single great vessel, usually termed the common trunk, arising from the ventricles. Also, it is known as persistent truncus arteries, truncus arteriosus communis, common aorticopulmonary trunk
Truncus Arteriosus - Classification
The first classification was published in 1949 by Collett and Edwards, they classified the anomaly to IV types depend on the origin of the pulmonary arteries from the truncus artery. (see figure I)
on 1965, Vann Praaghs published another classification adding the absence of the ventricular septal defect as group B (see figure I)
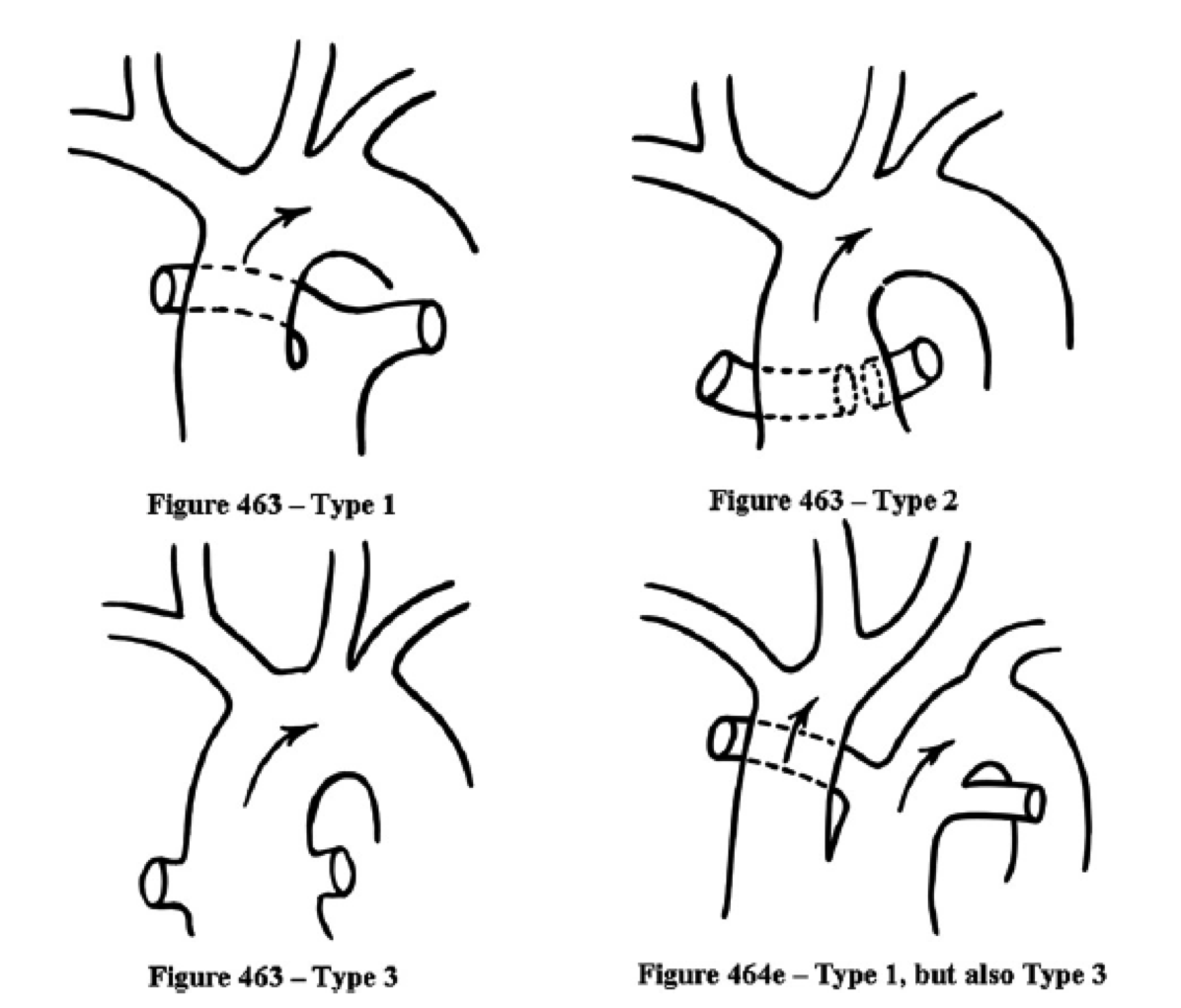
Recently in 2011, Russell et al published a simplified method to classify this anomaly after revising 28 autopsies (Figure II)
Figure 1
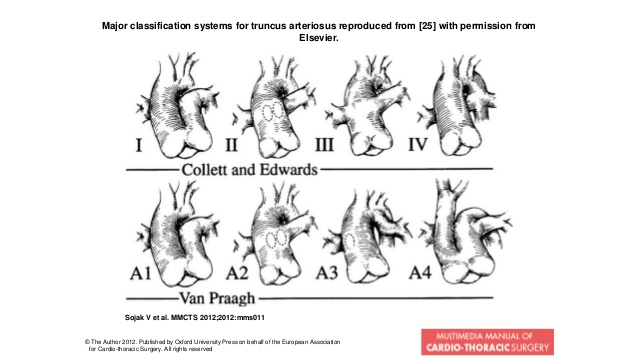
Figure 2
Truncus Arteriosus - Associated Anomalies
- Right aortic arch 25%
- Aberrent subclavian artery in 10%
- Interrupted aortic arch 10%
- TAPVR
Truncus Arteriosus - Pathophysiology
- In the early neonatal period usually the babies are asymptomatic due to high pulmonary vascular resistance (PVR) with semi-balanced circulation and arterial saturation 75-80% and episodic cyanosis. When the PVR starts to fall down after the first week of life the saturation will start to increase with the starting of pulmonary overflow and heart failure symptoms if there is no stenosis in the pulmonary arteries.
Usually, if the patient can tolerate heart failure in the first two months the PVR will start to increase and the symptoms may reduce, but they will be prone to irreversible pulmonary hypertension by 6 months of age.
- Additional feature may appear depend on any associated anomaly (like truncal valve stenosis or regurgitation, etc.)
Examination
- Signs of heart failure including gallop rhythm some times.
- A prominent left parasternal systolic murmur
- Aortic early diastolic murmur
- Continuous murmur is noted occasionally and is most often due to stenosis at the origin of one or both pulmonary arteries.
Truncus Arteriosus - Symptoms
Neonates usually presenting with tachypnea, tachycardia, irritability, and unwillingness to take either breast or bottle feedings during the early weeks of life, all manifestations of heart failure.
Infants who survive for longer periods, recurrent respiratory infections, dyspnea, and failure to thrive are usually present, and cyanosis is more apparent secondary to rising PVR.
Older children may occasionally present with increasing cyanosis (Eisenmenger syndrome).
Electrocardiogram
usually not specific and may show slight right axis deviation or biventricular hypertrophy
Chest X-ray
- Moderate cardiomegaly with pulmonary plethora
- Narrow superior mediastinum
- Right sided aortic arch in 20-40%
Echocardiography
- is considered as gold standard in diagnosis and is sufficient to define the relevant anatomy for management planning
- For truncal valve usually assist in parasternal short axis with apical and subcostal views (for anatomy, valve regurgitation or stenosis)
- outlet ventricular septum
- origin of right and left pulmonary arteries via parasternal view
- Both coronary arteries need to be well examined for any associated anomalies
- Finally; examination of the aortic arch for sidedness and any anomalies (interrupted aortic arch) with focusing on suprasternal notch view.
Cardiac Catheterization
- The need is limited to selective cases, specially late presenting patients.
- Mainly to determine the pulmonary bed resistance
CT/MRI
- Rarely needed, but preserved for selective patient with unanswered questions from previous imaging modalities.
Medical Management
The rule of medical management only to stabilize the general condition of the newborn for 24-48 hrs before surgery
Indication For Surgery
The diagnosis of TA is an indication for surgery per se, once the diagnosis made, the preparation for surgery started and the baby to be stabilized medically for 24-48 hrs
Timing For Surgery
- Once the diagnosis is made.
- In first week of life for the prenatal and neonatal diagnosed babies
Surgical Repair
- Including closing of ventricular septal defect, using autologous pericardium or synthetic patch
- Separation of pulmonary arteries from the truncal artery.
- Establishment of the continuity between the right ventricle and the pulmonary arteries by the right ventricular to pulmonary arteries valved conduit.
- In some cases, reconstruction of the pulmonary arteries may be needed.
- the repair becomes more complicated in cases associated with interrupted aortic arch and in Type IV Collett-Edwards (A-IV Vann Praagh) which consider as a type of MAPCAs (Major aortopulmonary collateral arteries)
The Result Of Surgery
- Current expected hospital mortality for neonatal repair of truncus ranges between 4.3% and 17%, with the majority of deaths occurring in complex truncus arteriosus
Early Post-operative Period
- Junctional ectopic tachycardia
- High PVR
- several manifestations of DiGeorge syndrome that may become clinically relevant in the postoperative period.
Long Term Follow-up
For:
- Progressive pulmonary vascular disease even after neonatal repair.
- Progressive truncal valve regurgitation
- Conduit replacement due to stenosis or severe valve regurgitation
1. Collett RW, Edwards JE. Persistent truncus arteriosus: a classification according to anatomic types. Surg Clin North Am 1949;29:1245–57.
2. Van Praagh R, Van Praagh S. The anatomy of common aorticopulmonary trunk (truncus arteriosus communis) and its embryonic implications. A study of 57 necropsy cases. Am J Cardiol 1965;16:406–25.
3. Jonas, Richard A. Comprehensive Surgical Management of Congenital Heart Disease, Second Edition, 2nd Edition. Truncus Arteriosus (Jonas 571).
4. KIRKLIN/BARRATT-BOYES Cardiac Surgery , 4th Edition.
5. The Natural and Unnatural History of Congenital Heart Disease J. I. E. Hoffman, 1st edition 2009.
6. The textbook of Pediatric and Congenital Cardiology, Cardiac Surgery and Intensive Care, Eduardo M. da Cruz Dunbar Ivy and James Jaggers. 1st edition.
7. A simplified categorization for common arterial trunk Russell, Hyde M. et al. The Journal of Thoracic and Cardiovascular Surgery , Volume 141 , Issue 3 , 645 - 653.